

Systemic Musculoskeletal Biomechanics - based on the Mezieres Method
Dr. Mauro Lastrico
Mezieres Method
The Mézières method identifies mechanical joint conflict as the cause of symptom onset.
Mechanical conflict, if not caused by congenital or acquired structural alterations, is determined by the progressive asymmetric shortening of acting muscles, following dominant vector force lines.
Muscle shortening initially involves the contractile portion, with increased basal tone.
By force and contraction time, the connective part of the fiber will also be affected, resulting in residual myofascial shortenings.
The involvement of both components produces an increase in the muscle's resistant force.
Objectives
The method's goal is to act on the symptom by restoring the physiological joint sequence, reducing excessive basal tone, and lengthening the muscle's connective portion.
In this way, the resistant force decreases but, at the same time, Work capacity (force times displacement) and Power (Work expressed per unit of time) increase.
The differentiation between resistant force, work, and power is the key concept of the entire evaluative and therapeutic approach.
The resistant force of a muscle (resistant to traction, i.e., stretching) is increased by the increase in basal tone, by any contraction bringing insertion points closer, by isometric contractions not in maximum physiological or relative fiber elongation, and by eccentric contractions.
The amount of increase depends on the force/time of execution/holding.
The effect on the skeleton is greater stability but, at the same time, greater rigidity with consequent compression on the joints: the balance between static and dynamic components shifts in favor of the static ones.
The capacity to develop Work is proportional to the insertion distance (Work = force times displacement), i.e., the amount of travel the muscle performs during contraction.
Power is a parameter that informs about the amount of time used by Work.
Work and Power are closely linked to muscle elasticity, basal tone, and balance between agonists and antagonists.
Restoring the length of retracted muscles means increasing their capacity to develop Work and Power and, consequently, bringing the balance between static and dynamic components closer to its ideal state.
The therapeutic action will be both analytical and systemic: analytically it acts on individual muscles or muscle groups responsible for specific skeletal alteration; systemically it aims to recover the body's overall center of gravity and to create conditions so that it is no longer necessary for the patient to use non-physiological movement strategies.
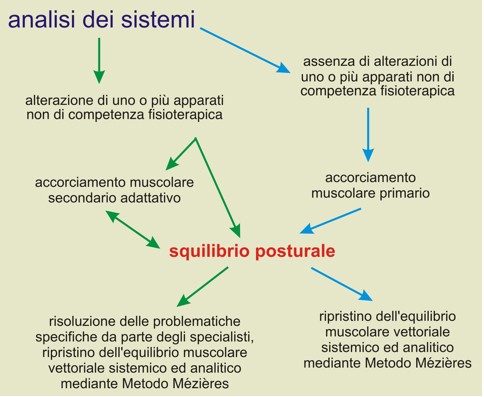
Schematically, the symptom can be:
- expression of a specific pathology not attributable to local or systemic muscle shortening: in this case resolution of the problem is beyond the therapeutic possibilities of the Mézières method and specific medical or physiotherapy methods must be used
- expression of a local dominant muscle shortening: the goal is to restore the physiological joint succession through the analytical vectorial rebalance of locally acting muscle forces, preventing systemic compensations and worsening
- expression of primary or secondary systemic muscle shortening, originating from or causing postural imbalance: in this case postural analysis will be used, checking for possible alterations from subsystems not related to physiotherapy, and analytical and systemic vectorial muscle rebalancing
Tools
The increase in muscle resistant force is determined both by the increase in basal tone of the contractile portion and by the shortening of the connective portion.
The means used aim to act on both components.
- Contractile portion: relaxation techniques, proprioceptive techniques, and decontracting massage techniques are used.
- Connective portion: the preferred technique involves the use of isometric contractions at maximum physiological or relative fiber elongation. For muscle groups where isometric contraction is not possible, stretching is used. In addition, manual deep massage techniques along the direction of muscle fibers are used.
Effects of isometric contraction
Isometric contraction produces elongation of the connective portion only if performed at maximum fiber elongation.
Maximum elongation will be relative to the maximum elongation capacity of the treated muscle and therefore not necessarily coincident with the maximum physiological elongation.
However, if isometric contraction is performed below the available maximum elongation, the consequence will be further shortening of the connective component.
See the articles on "muscle mechanics" for more on this.
Using a simplified fiber behavior mathematical model, during an isometric contraction at maximum physiological or relative elongation it occurs: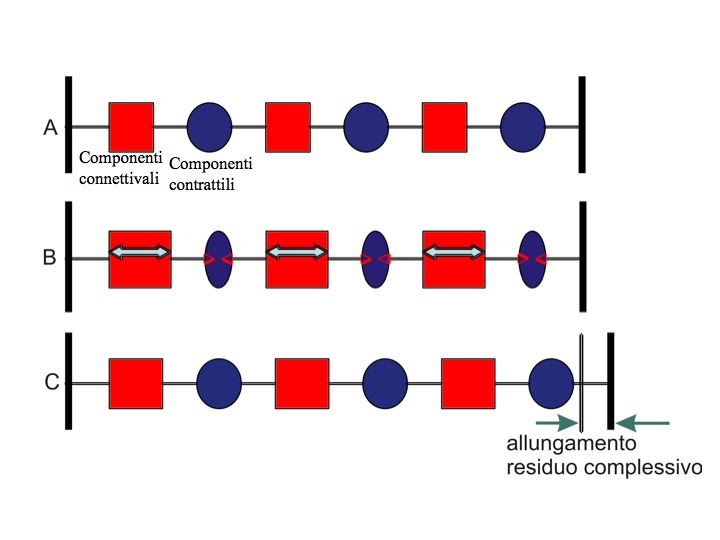
"A" represents the muscle fiber at maximum physiological or relative elongation; "B" active contraction: the contractile portions in blue actively shorten and exert a traction on the connective parts in red; in "C", at the end of contraction, depending on the force and contraction time, each connective component will have undergone elongation deformation and the green arrows represent their sum.
The contractile portions will undergo shortening deformation instead, but since their elasticity coefficient is higher than that of the connective portions, the residual shortening of the contractile portions will be less than the residual elongation of the connective portions.
To resolve the residual shortening of the contractile portions, it will be sufficient to use a relaxation technique at the end of contraction. The contractile portion, in fact, does not undergo actual shortening but rather an increase in basal tone.
Execution modalities
Once the objectives, both analytical and systemic, of the treatment have been identified, corrective strategies are applied using the means described above.
The corrective maneuvers, besides addressing the affected district, must be such as not to have aggravating components in any other body district.
Example: a patient might have a high shoulder caused by the retraction of the ipsilateral cranio-cervico-scapular muscles.
As corrective action, one could choose to use the skull as a fixed point and ask for active lowering of the shoulder.
This modality is effective for the upper trapezius bundle, but lowering the shoulder causes the scapular insertion of the levator scapulae and omohyoid muscles to move away.
If these muscles are shortened, they will exert a pulling force on the cervical vertebrae (levator scapulae) and on the hyoid bone (omohyoid).
If the patient already has cervical vertebrae with lateral convexity on the side of the high shoulder, the final result of the therapeutic action would be an improvement in shoulder position but a worsening of the vertebral convexity.
From a therapeutic point of view, such a result would be a serious mistake, with potential symptomatic repercussions.
The asymmetries present represent, for the patient, the best possible balance, with adaptations aimed at minimizing conflicts.
When deciding the therapeutic intervention, it is necessary to create conditions so that the new balance is overall better than the one spontaneously adopted by the patient.
Moreover, in the presence of emerging abilities, theoretical maneuvers are not always effective, and it is therefore necessary to seek the subjective adaptive modalities specific to each patient.
A patient might present, for example, a dorsal hypokyphosis at D5 apex due to retraction of the scapular adductors.
Therapeutically, one could actively ask for protraction of the shoulders using the physiological motor muscle, the pectoralis major.
By protracting the shoulders, the scapulae abduct putting the scapular adductors in passive stretch, and the dorsal spine is projected posteriorly.
However, if the pectoralis majors are replaced by the latissimus dorsi-upper trapezius bundle, protraction will occur with elevation of the shoulders and internal rotation of the humerus.
The effect will be that the dorsal vertebrae projected posteriorly will have their apex between D7 and D12, while D5 (physiological apex of dorsal kyphosis) will further decrease in kyphosis.
Thus, a dorsal curve inversion and an increase in cervicodorsal lordosis will occur.
In this case, to make the therapeutic action effective, it is necessary first to identify and intervene on muscular substitutions, creating conditions so that the patient is no longer forced to use them.
Therapeutic modalities must therefore be differentiated according to the subject's characteristics and take into account the entire static and dynamic examination.
Apparently similar dysmorphic patterns can be supported by completely different vectorial muscular alterations.
Within the therapeutic pathway, the choice of strategies to achieve objectives is therefore conditioned by many variables that make exhaustive treatment impossible within this writing.
Conclusions
In summary, the Mézières Method is an active rehabilitation technique consisting of individualized treatments differentiated according to the specific therapeutic needs and subjective characteristics of each patient.
Through relaxation and lengthening of the retracted musculo-fascial kinetic chains, it induces a morphological modification of the body, bringing it, proportionally to the number of treatments performed, closer to its ideal form.
The field of interest is orthopedic pathology:
- vertebral (scoliosis, hyperlordosis, hunchback, intervertebral disc compression and related radiculopathies, sciatica, cervico-brachialgia, etc.)
- articular (osteoarthritis, scapulo-humeral conflict, coxarthrosis, etc.)
- muscular (low back pain, torticollis, myalgias, etc.)
- dysmorphic (temporomandibular locking or subluxation, winged scapulae, varus or valgus knees, flat or hollow feet, hallux valgus, etc.).
Experiments of the technique in neurological pathologies have shown that the Mézières method can be used as support for specific rehabilitative techniques.
The goal is to limit the appearance of orthopedic alterations which, combined with neurological ones, would increase the patient's discomfort.