Macrì Giuseppe Fkt and D.O ; Macrì Pasqualino Fkt and D.O ; Panero Antonella Speech Therapist The increasingly deep study in recent years in the rehabilitative medical field on human posture has revealed many innovative theoretical aspects that are leading to the refinement of concepts and related rehabilitative practices of kinesiology methods in use.
We are witnessing the emergence of new concepts based on: - A global vision of the subject
- A search for myofascial causes outside the painful area
- A constant and overlapping (spatial-temporal) interaction between posture and human dynamics as a result among the various functional systems
- Recognition of synergies among the various muscle groups (myofascial chains)
- Interpretation of sense organs as bi-directional transducers between the cyclical metabolic needs of the human body and its environment
- A constant gestural and attitudinal communicative relationship between the human body and the external environment, a determining factor in the strategy of posture choice by the individual
- A transient or permanent conditioning of postural attitude by the psychological state of the subject, through its bodily somatization.
fig.1 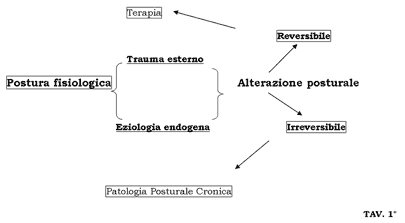
The study of posture, in its evaluative meaning, cannot disregard for the subsequent rehabilitative approach the nature of the etiological form (acute or chronic) that disturbs the subject's static that we are examining (see table 1).
The causes that modify the static and the consequent postural dynamics can be differentiated into exogenous (external traumas) and endogenous (antalgic compensatory attitudes, structural, dysfunctions of the physiology of sensory systems, etc.).
Further differentiation is that with the character of reversibility and irreversibility (in relation to etiology, age, metabolism, musculoskeletal structure, surgical trauma, etc.). This assessment is a sine qua non condition in choosing the subsequent therapeutic strategy.
In their extreme complexity, all apparatuses are necessary to allow the maintenance of the upright position, walking, running, postural transitions, etc... but there is certainly a predominance or "specificity" of function. As biology teaches, every type of function is present in the cell, but its belonging to a tissue highlights the dominant function (contractile function, conduction, transport, etc.) in relation to the task the tissue must perform within the organ. We could take for example the neurological automatisms of subcortical origin (therefore unconscious in nature) which are the basis of voluntary (conscious) acts in the performance of any movement: without these automatisms structured during our ontogenesis, our fine manual skills, the ability to flee or even the "simple" walk would not be achievable. Everything we perceive about movement is only the tip of the iceberg: it is only the final result of a huge amount of chemical-physical mechanisms inside the body starting at the cellular level.
All this requires balance in the maximum possible metabolic economy: it is a biological survival law that concerns the entire animal world. But man certainly has an extra weapon for his survival and it is the possibility to communicate with his peers at a higher level, namely to metacommunicate.
Vocalization is allowed thanks to structures that have adapted to an anti-gravity evolutionary character. Human posture is in function of vocal and gestural communication. Let us then try to describe the role of the hyoid bone in the physiology of posture and its synergistic action with other distal structures to it or belonging to other apparatuses. Anatomically the hyoid bone is a horseshoe-shaped bone with two small protrusions on top called small horns. The portion delimited between the two small horns medially is the body of the hyoid: the remaining equal and symmetrical parts that extend postero-laterally are the great horns. Only in adulthood the various parts that compose it weld together (table 2). fig.2 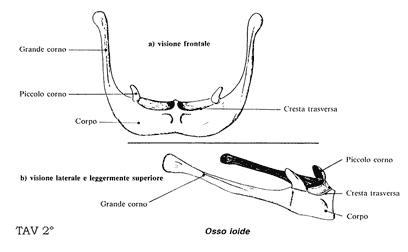
In the first decades of life the small and great horns are articulated with the body in order to meet the needs of infant growth. It will weld in mature age and will be mainly made of compact bone.
Topographically it is positioned supero-anteriorly to the thyroid cartilage of the larynx and infero-posteriorly to the mandible. It is connected through muscular, ligamentous and membranous connections to many mobile structures of the human body. It should be noted that there is space on it for 24 equal and symmetrical muscular insertions and 9 membranous-ligamentous insertions: by comparison we can take the coccyx on which 4 muscles insert (Testut–Latarjet). This gives us a first idea of the balancing role it plays in local dynamics.
It is related to structures performing different but extremely mobile functions.
In this regard see the diagram in figure table 3.
The vector algebraic sum of the tensions of the muscles, ligaments and fasciae that insert on the hyoid bone and depart from it determine the physiological horizontal position of the hyoid, essential for the roles entrusted to it.
It is a pivot point serving mastication, swallowing and phonation.
In phylogeny the hyoid bone appears practically in its bony structure, morphologically simpler than the human one, in reptiles in which pulmonary respiration is given the full task of respiration (in amphibians such as salamanders or frogs for example it is not in the complete form and respiration is also entrusted to the cutaneous apparatus). Reptiles are that class of animals "completely emerged" from the aquatic environment in which the engine of respiration (having become completely pulmonary) is represented by the rib cage. Also, although the thyroid cartilage is not present (therefore absence of vocal cords) a few sounds or whistles are produced anyway in order to communicate among peers.
With mammals appear the thyroid cartilage and the epiglottis. The hyoid bone then takes on ligamentous and membranous connections with the cricoid ring, the thyroid cartilage and the aponeurotic raphe of the tongue. In humans it passes from a more cranial position (as seen in chimpanzees and human infants where it is necessary to feed and breathe at the same time) to a more caudal position (of the adult), dilating supero-inferiorly the pharynx to benefit a finer and more complex vocal emission.
Therefore we can note how the hyoid bone: - follows a structural and morphological evolution roughly in parallel to the displacement of the body center of gravity from the base of support
- can allow anatomical structures to evolve structurally and morphologically leading to a phonetically complex communication like the human one
- can have the task of preserving the larynx as a whole from compressions in twisting movements, flexion-extension or lateral inclination of the head in relation to the shoulder girdle.
fig.3 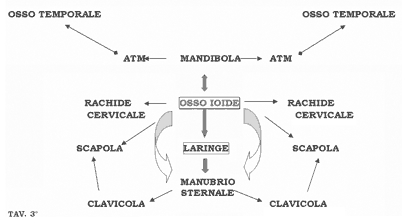
Keeping in mind its myofascial connections with other very mobile structures of the upper trunk and shoulder girdle (table 2), we can interpret the role of the hyoid bone as a distributor, a distributor of multidirectional vector forces. We can venture the idea of roughly assimilating the hyoid bone to a densified "phrenic center" (the bone is specialized connective tissue!). What sense would a bony structure have in an area with a predominant organ-visceral presence with such morphology if not to concentrate and distribute myofascial and pressure tensions of high power in relation to its volume?
It becomes a pivot point on which three-dimensional forces acting simultaneously can anchor, becoming a temporarily rigid point:
but it must also be able to move, to momentarily change position.
Here its role becomes essential in the mechanics of swallowing, chewing (in movements of opening, closing and lateral movement of the mandible) and in representing the pivot point in the articular dynamics of the laryngeal cartilages.
Through this last coordination which takes place at the chondro-articular and myofascial level it becomes possible to carry out the complex phonetic function and specifically the emission of pure vowels (a typical characteristic of the human being) and indirectly in the mechanics of the vocal tract and the bucco-labial system. The physiology of the bilateral thyro-cricoid and crico-arytenoid joints depend on the ability of the hyoid bone to attract on itself the antigravity forces that develop during postural transitions.
Besides vocal function it is also indispensable in mastication. In fact it is rightly said about occlusion and temporomandibular joint in posture, but little attention is paid to the hyoid apparatus. In this action it "returns the courtesy" to the tongue and mandible, becoming a fixed point of the suprahyoid muscular system engaged in mastication and therefore in the active opening of the mandible.
Swallowing represents an important function for the upper airways and digestive tract. In this there is again a very close synergy with important anatomical structures also from a postural point of view as seen above.
In this function the mandible stabilizes on the maxilla normally with a centric occlusion; the tongue exerts its balanced force on the palate and on the palatal surface of the upper arch teeth. An interesting anatomical fact for this analysis is to note how the tongue is not a single muscle but a muscular complex composed of 16 smaller muscle bellies. Therefore, alterations of tongue dynamics influence in the medium and long term the horizontality of the hyoid bone and its various as well as synergistic physiological actions.
Also in various scientific studies on muscle-ligament chains conducted by various authors we find the hyoid structure within a specific functional chain. But what stands out most is to see how the hyoid apparatus, directly or indirectly, represents a crossroads of vectors of various kinetic chains.
Taking for example the studies of PIRET and BEZIERS (1986) we see that they identified five muscle chains with the particularity of starting
intracranially from bone-meningeal force lines. Outside the skull they materialize in muscles, ligaments and bones interposed to them. The hyoid is inserted in the lingual chain that materializes on the sagittal plane with an anterior multi-vector chain connecting the mandible to the pubis and perineum. But through its ligamentous connections, it is related to other chains such as the pharyngo-prevertebral and masticatory.
Other authors have studied and drafted different types of dynamic functional chains, including deeper fascial structures, but the great interest that these researches have is to arrive at some considerations. A) The physiology of myofascial chains is at the service of both posture and motor skills (understood as the sum of mobility and motility of the body): they are two sides of the same coin.
B) Furthermore these functional chains lend themselves perfectly to a biological analysis considering them as a whole as open complex systems (O.C.S.).
1) "All forces acting in the system are interdependent"(including the hyoid bone)
2) "Understanding the functioning of an O.C.S. can only take place through understanding the O.C.S. as a whole" (the concept of structural and functional globality: all for one, one for all)
3) "The O.C.S. are capable of generating original solutions that are not given by the simple sum of the forces acting" (in the functional and/or structural specificity there remains a fundamental multifunctional capacity.)
C) How much physiology and anatomy are interdependent: structure supports function (it is the musculoskeletal structure that allows movement), but in turn function shapes and maintains structure (correct physical activity). With reference to the explanatory note of table 1 and more precisely regarding the irreversible aspect of postural pathology, we can grasp the importance of the hyoid function in patients who, following neoplastic pathology, undergo surgical intervention of the larynx and consequently of the hyoid, the ipsilateral sternocleidomastoid muscle and the base of the tongue.. But this pathology will be the subject of a forthcoming work.
We hope that all this can be a useful stimulus to a broader and multidisciplinary research for the benefit of our professional knowledge and a greater effectiveness of kinesiology methods for better psychophysical well-being of our patients. |
|
Copyright © 2026
AIFiMM Formazione
Mézières Provider E.C.M. n. 1701. All rights reserved.
|

