

Mezieres Method: Postural Alterations According to the Psychosomatic, Neurophysiological, and Biomechanical Model
Dr. Mauro Lastrico
Posture:
psychosomatic, neurophysiological, biomechanical model
Dr. Mauro Lastrico, physiotherapist.
Excerpt from:
"Musculoskeletal biomechanics and Mézières method"
Author: Dr. Mauro Lastrico
Marrapese Publisher
Posture can be understood as the body's position in space and the spatial relationship between skeletal segments, aimed at maintaining balance, both in static and dynamic conditions, involving neurophysiological, biomechanical, psycho-emotional, and relational factors.
Consequently, posture can be studied through each of the following interpretive models: the psychosomatic model, the neurophysiological model, and the biomechanical model.
The psychosomatic model.
Around the 1920s, the first formulations by W. Reich and later A. Lowen on the deep relationship between psyche and soma, between character structure and muscular structure, emerged.
In his early writings, Reich, a physician and psychoanalyst, student of Freud, gradually affirmed the functional identity between psychic processes and somatic processes, relating character structure to the bodily structure of the person.
Tensions accumulated in the body and the enactment of attitudes aimed at blocking one's emotions, according to the scholar, give rise to a dual armor.
It is a character armor, understood as the set of psychic and behavioral attitudes characteristic of an individual, which has a somatic counterpart in muscular armor.
These structures function as a defense apparatus against internal and external stimuli perceived as threatening by the subject, aiming to avoid feelings of anguish.
Also described in orthopedics as "psychogenic myotensive state", the state of chronic muscular tension represents perhaps the most evident process by which the Ego expresses its emotional experiences in the body.
Alexander Lowen deepened research in this field and formulated a real therapeutic procedure called Bioenergetic Analysis. He studied the relationship among cognitive, emotional, and bodily levels specific to each person, focusing on skeletal functions and voluntary musculature. Psychophysiologically, muscular tensions represent the Ego's primary defensive tool expressed corporeally and can determine an overall shaping of postural attitude.
It can therefore be stated that muscular structure also reflects an individual's personal history.
The relationship between posture and personality is now supported by numerous scientific researches by scholars from various schools.
It is important to remember that to represent each individual in their psychosomatic unity, alongside musculo-tensive and postural aspects, it is essential also to refer to psychoneuroendocrine factors, considered as the mediating and modulating system between psychic-emotional components on one side and organic-biological factors on the other.
The formation of bodily armor occurs through an increase in basal tone, that is, an excess tension of the contractile portion of the muscle fiber.
If this persists over time, the connective portion is also affected, resulting in an actual shortening of the muscular system that will cause alteration of the correct articular sequence. Thus, an emotion-driven myotensive state can evolve and associate with a biomechanical problem.
The neurophysiological model.
The postural tonic system, regulator of muscle tone, is a cybernetic system within which a complex series of psychoneurophysiological processes occur.
In this system, incoming information from specific postural receptors (foot, eye, stomatognathic apparatus, skin, musculoskeletal apparatus, etc.) influences the output, namely muscle tone.
However, this output conditioning is itself the result of processing of the sensory inputs by neuropsychological and experiential processes.
Therefore, a postural imbalance does not necessarily indicate a problem originating at the sensory input level, but can be linked to improper central integration: cortical centers identify static or dynamic goals while subcortical centers, using a mapping called "body schema", implement executive strategies. Cortical centers identify the "what", subcortical centers the "how". Furthermore, subcortical centers regulate basal tone via the gamma circuit.
Being the "what" prioritized over the "how", the subjective representation of the body schema determines the quality of muscle use: the less well the body schema is represented, the more the muscular system will be used in excessive tension, co-contraction of unnecessary muscles for the action, even to organize substitute moments, in which muscles anatomically assigned to a given action are replaced by others (emergent abilities).
Subcortical centers are also involved in defensive strategies aimed at life preservation through muscular contraction mechanisms distinguishable as "physiological" and "functional".
Muscle contraction, depending on force/time variables, determines residual muscle shortening: the shorter the contraction time and force, the smaller the shortening; the greater the force, especially the time, the greater the residual shortening.
Muscle shortening and resulting bodily asymmetry are not only found in people with orthopedic pathology/symptoms but are present in every human being and can be induced by automatic muscle contractions in response to an event.
In the following, "physiological" means those muscle contraction mechanisms every human uses in response to an event/stimulus; "functional" means those muscle contraction mechanisms every human uses with subjective variability in quantity and quality, answering the question "what I need".
Both mechanisms are controlled by subcortical centers.
Subcortical centers are phylogenetically ancient in human evolution and have primary tasks including adopting strategies useful for life preservation.
Physiological mechanisms
They are muscle reactions in sustained contraction following orthopedic traumatic events. Example: accidental event and tibio-tarsal sprain. Subcortical centers send, via gamma motor neuron, contraction signals to all periarticular muscles to immobilize the joint. This contraction lasts until injured intra-articular structures are "repaired". The duration of contraction corresponds proportionally to the damage; thus the residual muscle shortening.
Functional mechanisms
They are sustained muscle contractions, essentially an increase of basal tone, always activated by subcortical centers via gamma motor neuron, aiming to reduce or eliminate present pain (retrospective pain reflex) or to prevent latent pain manifestation (anticipatory pain reflex).
Sustained muscle contraction, as long as it does not cause structural conflicts, has an analgesic effect.
In their role of life preservation, subcortical centers operate with only one time frame: "here and now". Pain or functional impotence are perceived as "death" and avoidance strategies are adopted.
In this light,
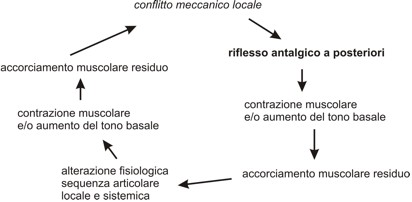
Retrospective pain reflex
represents the extreme defense mode to prolong life as much as possible. People in acute pain phase often assume twisted postures but, as patients say, they feel somewhat better.
This defensive strategy is useful initially but, if prolonged, becomes cause of further mechanical conflicts.
Physiological mechanisms and retrospective pain reflex intervene only at certain life moments and alone cannot explain the sum of shortenings and asymmetries in the body. These are mainly caused by the
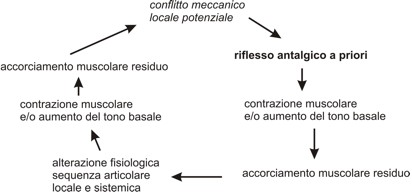
Anticipatory pain reflex.
It is a permanently active reflex aimed at preventing latent pain/mechanical conflicts from surfacing.
Progressive muscle shortening, as long as it does not create conflicts, prevents musculoskeletal discomfort from surfacing.
Subcortical centers use the muscular system distributing shortenings so as to systematically alter articular sequences trying to avoid local conflicts.
The anticipatory pain reflex also manifests through postural assumptions or movement, coercing the person into motor choices. Such coercions are initially unconscious: one "feels" the need/desire to move or position oneself in a certain way. If muscular shortening changes become greater, motor coercions become consciously aimed at avoiding discomfort (e.g. I cannot sit long otherwise..., I cannot walk slowly otherwise..., etc.)
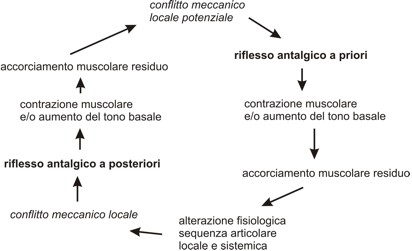
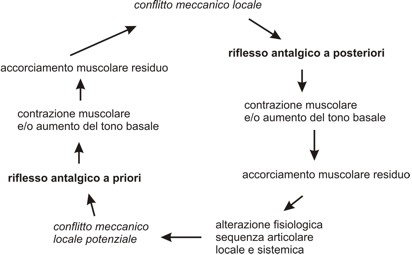
If the systemic muscular shortening mechanism persists, local conflicts may arise creating a self-feeding circuit where both pain reflexes coexist.
In conclusion, the living human body cannot adhere to the anatomical model also due to protective systems of the subcortical centers that allow living the "here and now" at best sacrificing the "then".
To do so, centers use the muscular system by increasing basal tone and/or muscle contraction creating an analgesic effect; if tension increase lasts enough time, it produces muscle shortening.
This will cause:
* systemic muscle shortenings
* analytical muscle shortenings of some dominant groups, by force vector, compared to others
* district and systemic alterations of physiological skeletal articular sequence
The biomechanical model
The biomechanical model analyzes how the musculoskeletal system "organizes" itself in statics and dynamics.
In statics, postural imbalances appear as loss of physiological articular sequence of skeletal segments in the three spatial planes; in dynamics as inability to perform movement optimally using muscular forces.
To ensure skeletal segment axiality and physiological joint movement, muscular forces must be balanced. Otherwise, application points of muscular force vectors, their moments, and load distribution on skeletal segments vary.
Regardless of primary disturbance elements and initial perturbation type, postural alteration results from interaction between the "complex system" muscular and "complex system" skeletal, giving rise to the functional interrelation "musculoskeletal complex system".
A localized perturbation causes initial misalignment and thus articular imbalance followed by muscle contraction with stabilizing function.
Conversely, correct articular sequence organization cannot ignore muscular tension balance.
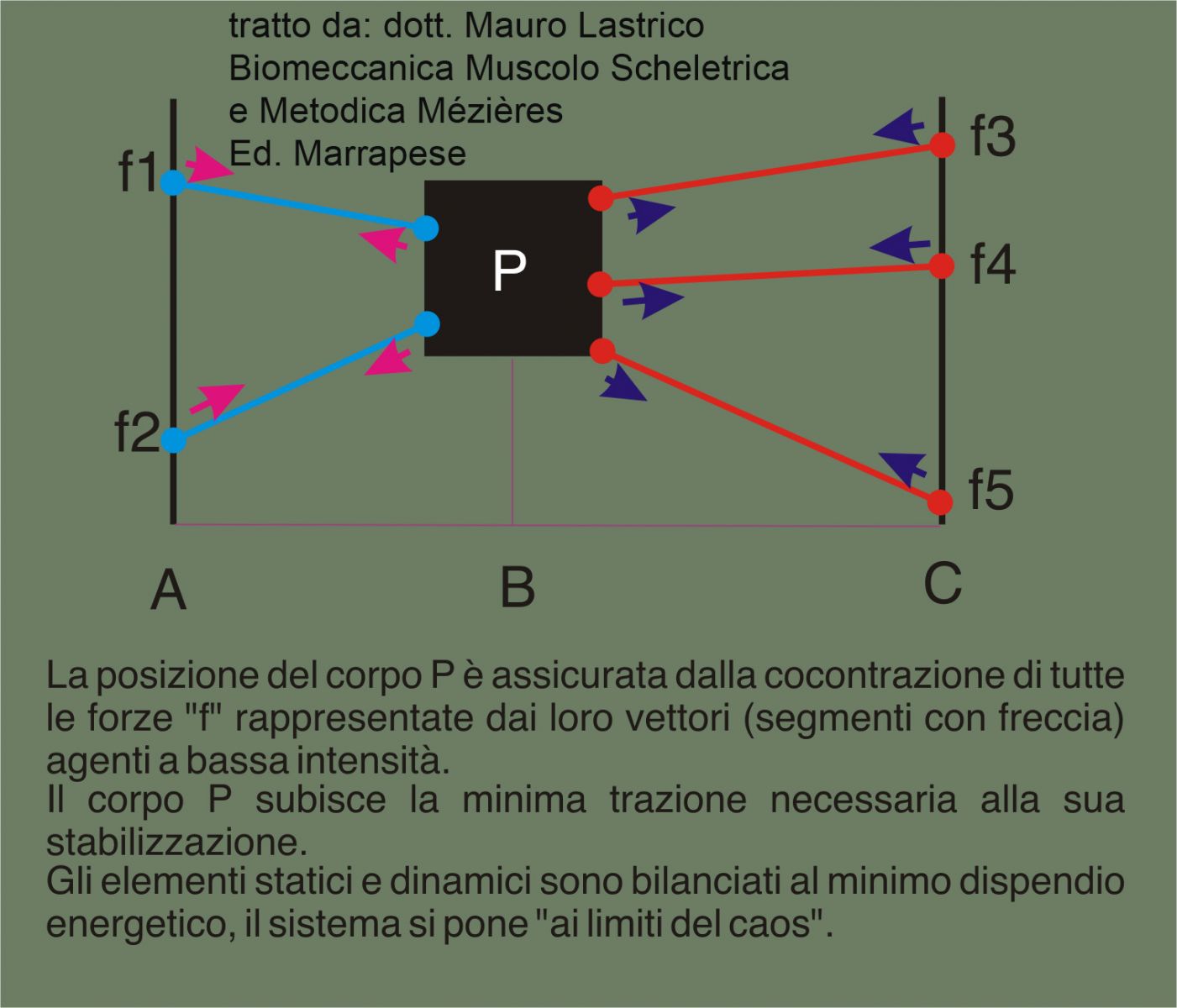
Low intensity equilibrium (muscle tone) of muscular vectors guarantees coexistence of good stability and joint mobility creating conditions for the musculoskeletal system to be "at the edge of chaos", the area where static and dynamic elements express optimally their structural potential.
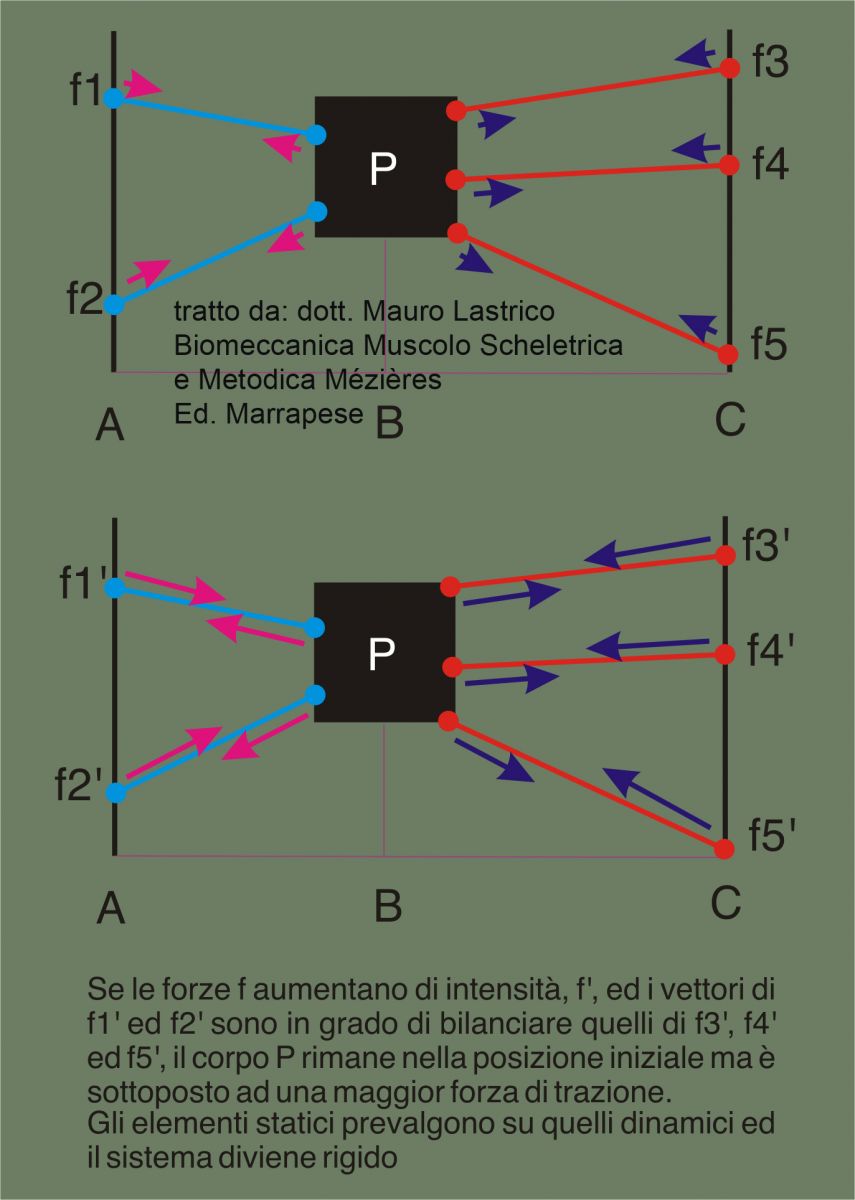
If force balancing occurs at high intensity, skeletal axiality remains possible, but movement requires more energy. Movement becomes disharmonic and skeletal components endure greater stresses. Static elements prevail over dynamic ones and system, moving away from the "margin of chaos", becomes rigid.
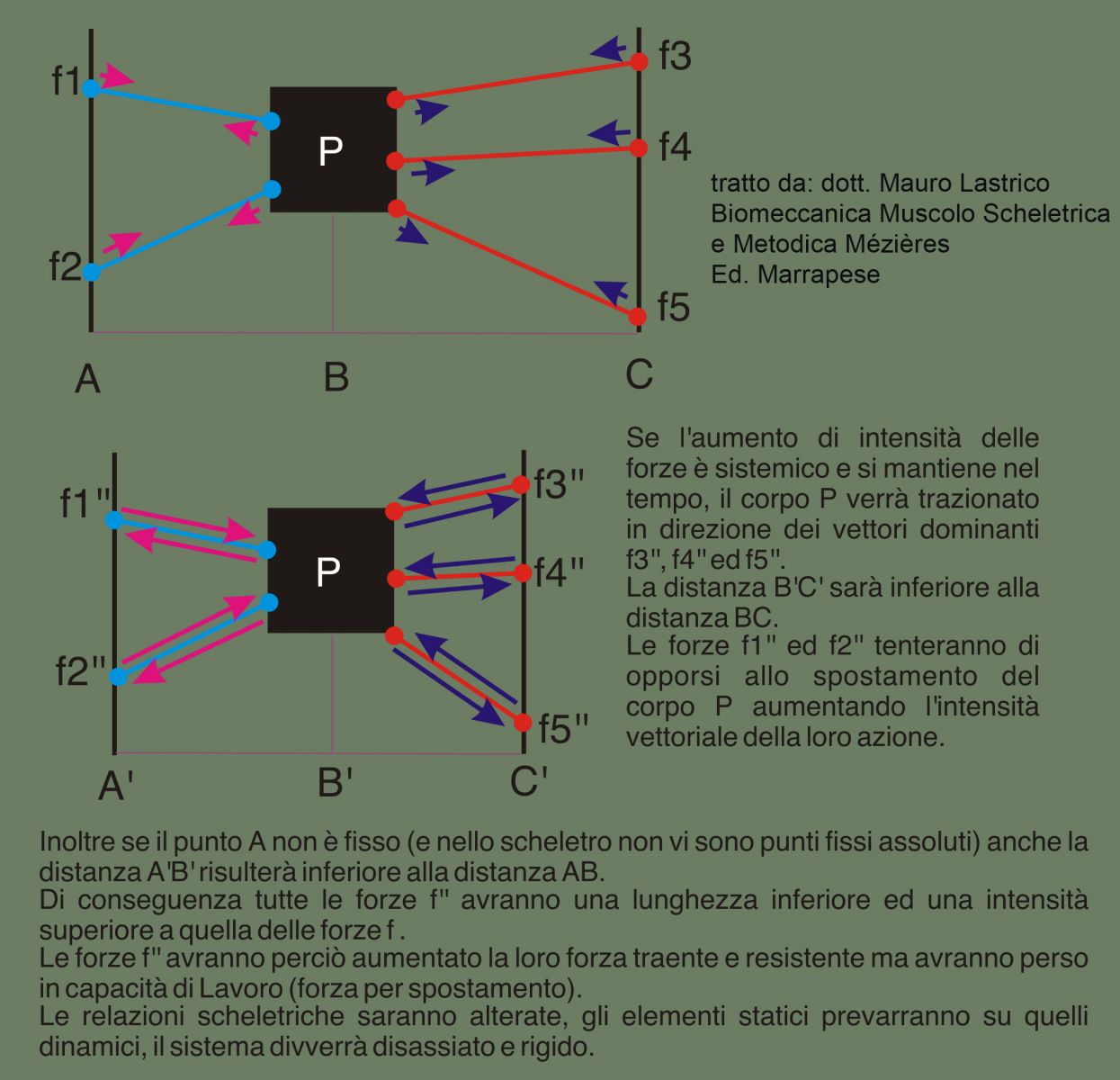
High intensity vector equilibrium (basal tone increase) over time provokes vector imbalance favoring dominant muscular forces and reorganization of a new adaptive equilibrium, at the cost of skeletal segment misalignments.
Movement will be limited or replaced by mobilization of other joints.
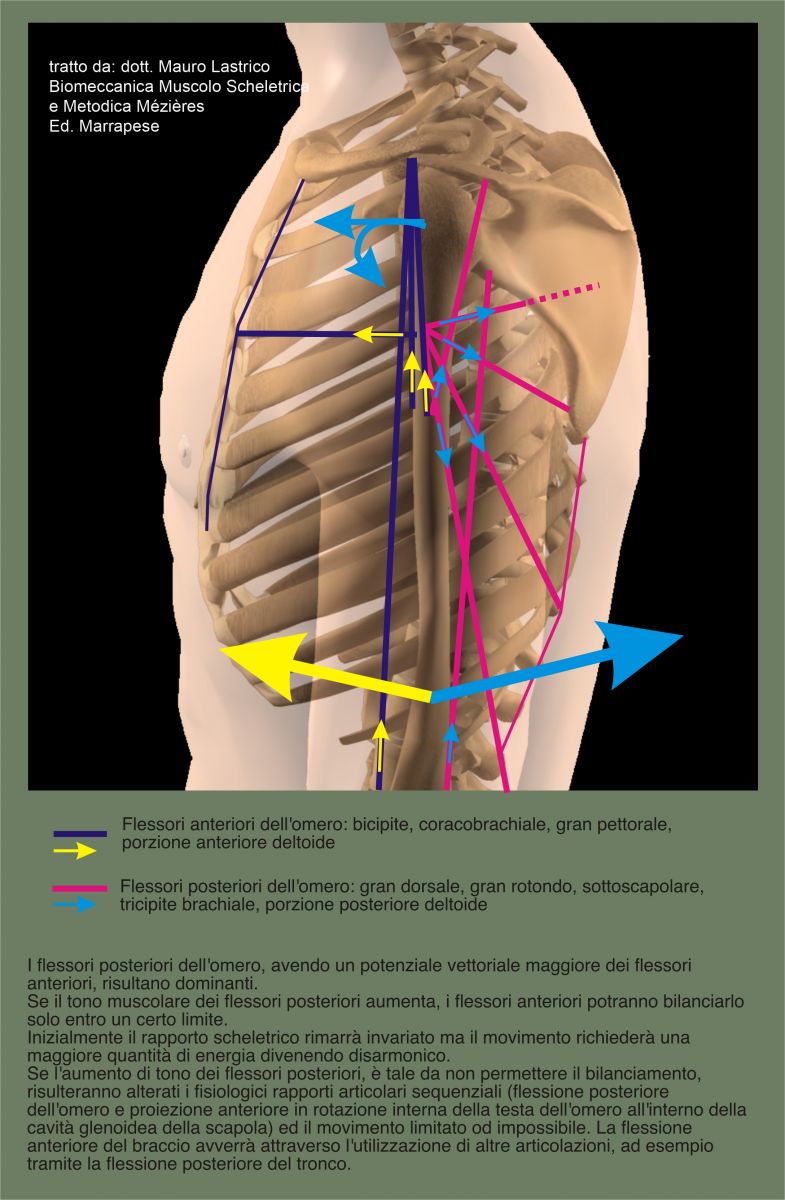
For example, considering muscles responsible for anterior and posterior humerus flexion, vector dominance—both in potential force and force line disposition—is in favor of posterior flexors.
This has static consequences (position of humeral head within glenoid cavity) and dynamic consequences in movement execution.
If muscle tone is physiological, force balancing ensures good joint relation and harmonic movement.
If tone increase allows anterior flexors to balance, humeral head position remains unchanged but articular structures endure more stress and movement requires more energy losing fluidity.
If tone further increases and contractures and shortening of connective muscle fiber occur, balancing may become impossible. Posterior flexor vector dominance alters joint relation by posteriorly flexing arm and anteriorly internally rotating humeral head in scapular glenoid cavity. Joint becomes rigid and intraarticular structures may cause mechanical conflicts.
Dynamically, anterior arm flexion will be limited and compensations like shoulder girdle elevation or trunk posterior flexion activate.
Skeletal alterations from muscle balance loss cause static and dynamic imbalances in body volume symmetry and motor functions, to which body schema must adapt. Movement effectiveness and utility will be guaranteed by compensatory schemes bypassing morphological or functional limits thanks to processing incoming kinesthetic sensations.
In upright posture maintenance, the postural tonic system aims to keep body barycenters and ground reaction forces within the support polygon given by feet surface.
In dynamics, the system uses gravity/ground reaction force couple to economize work needed for walking.
Overall barycenter results from summing individual skeletal barycenters.
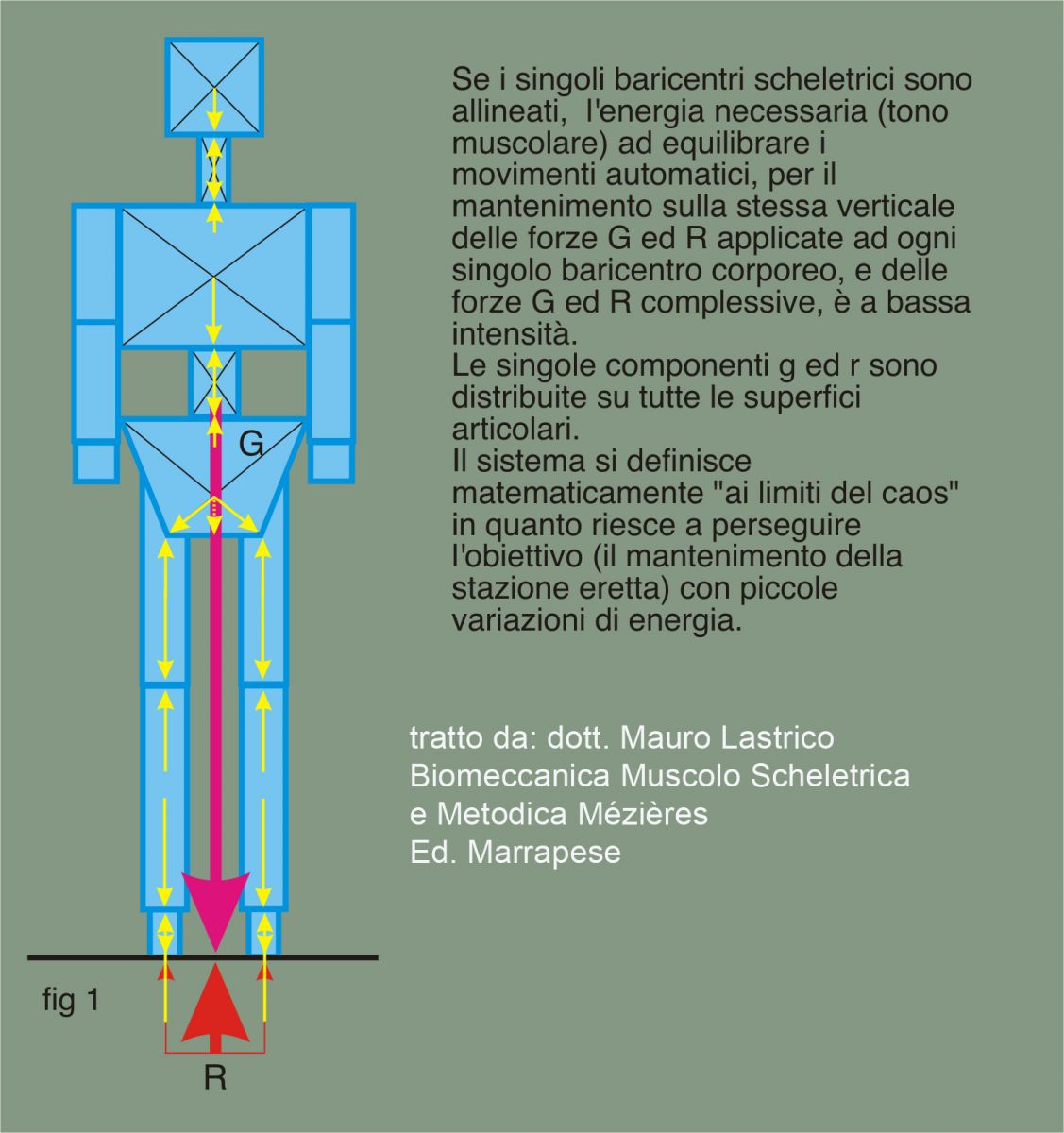
Simplifying the human skeleton as geometric shapes to ease barycenter calculation, it can be represented on frontal plane as in following figures.
In the first figure, basal tone—force developed by muscles maintaining individual body barycenters (mass centers), expressed as resultant force G, on vertical of ground reaction R (resultant joint reaction applied to support points)—is the minimum needed to counterbalance barycenter shifts induced by automatic body movements, e.g. breathing. Note that, though not shown with equal length segment, force R equals and opposes G: R = -G. Also, as skeletal barycenters are aligned, applied forces G and R have components g and r distributed over entire support surface. Joints thus work optimally without concentrated compressive moments on small areas. See "equilibrium of bodies" for g and r definitions.
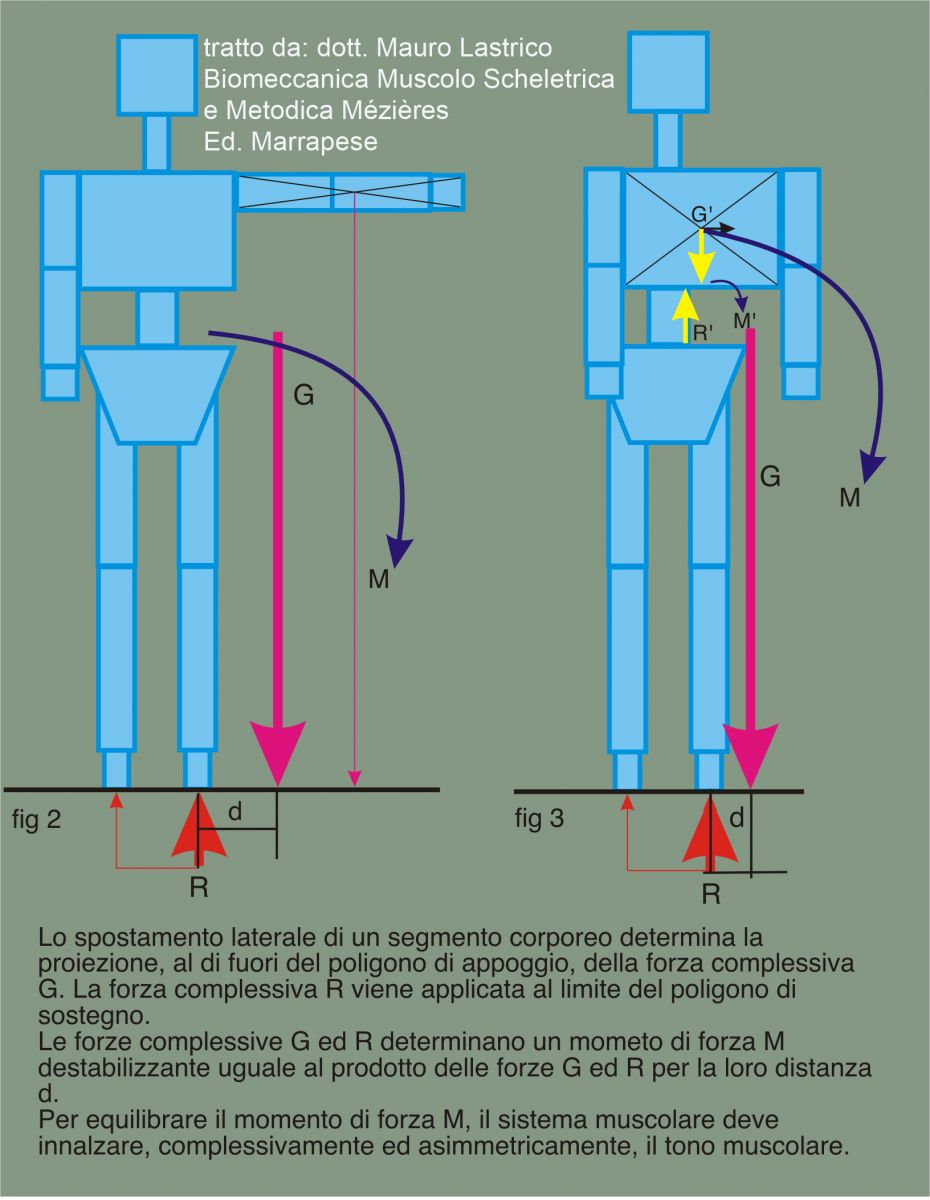
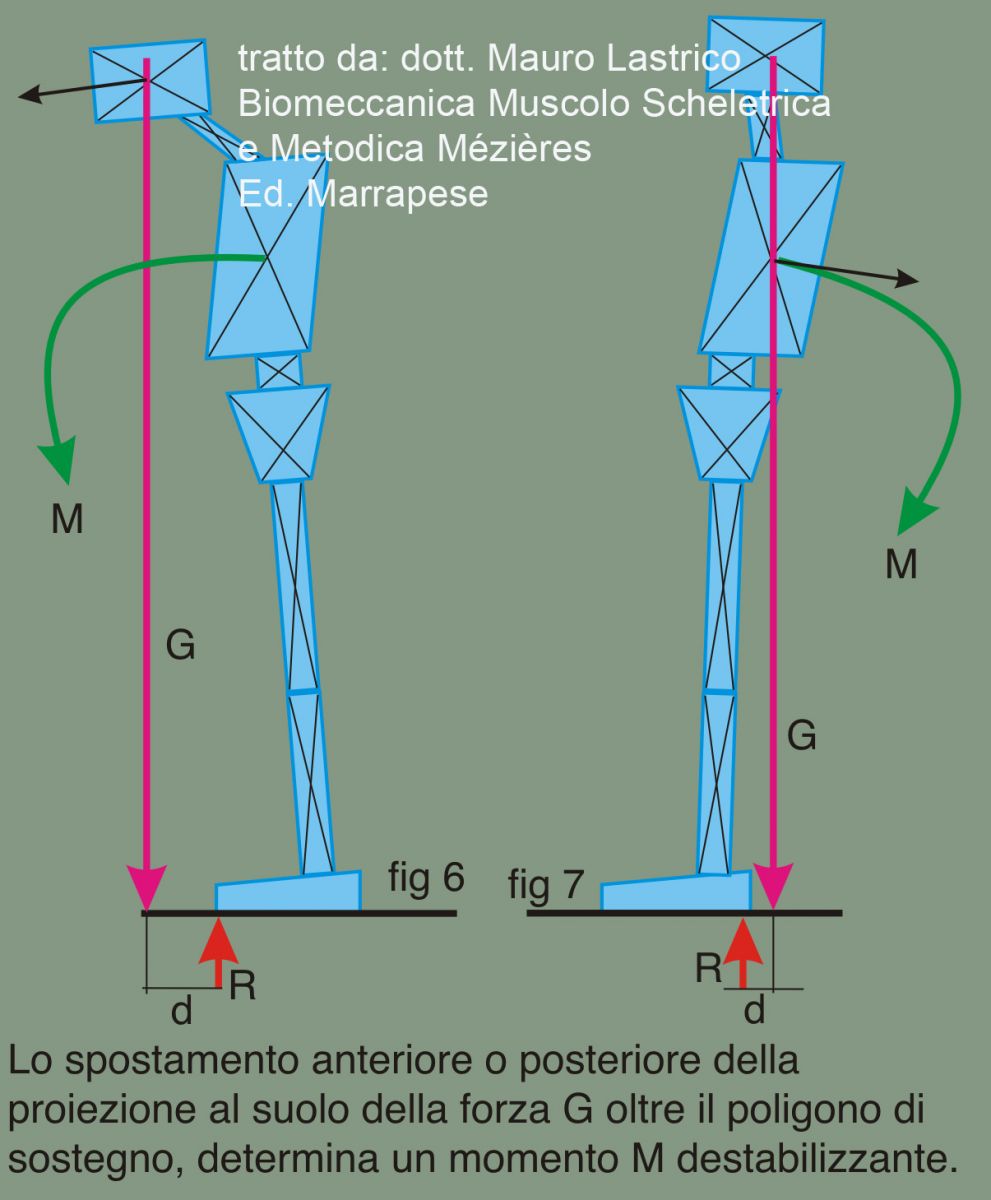
In following figures, lateral displacement of a body segment causes overall force G to "fall" outside support polygon. Resultant force R applies at polygon edge, creating destabilizing moment M given by forces G and R times their distance d.
Maintaining upright posture requires asymmetric co-contraction of muscular system.
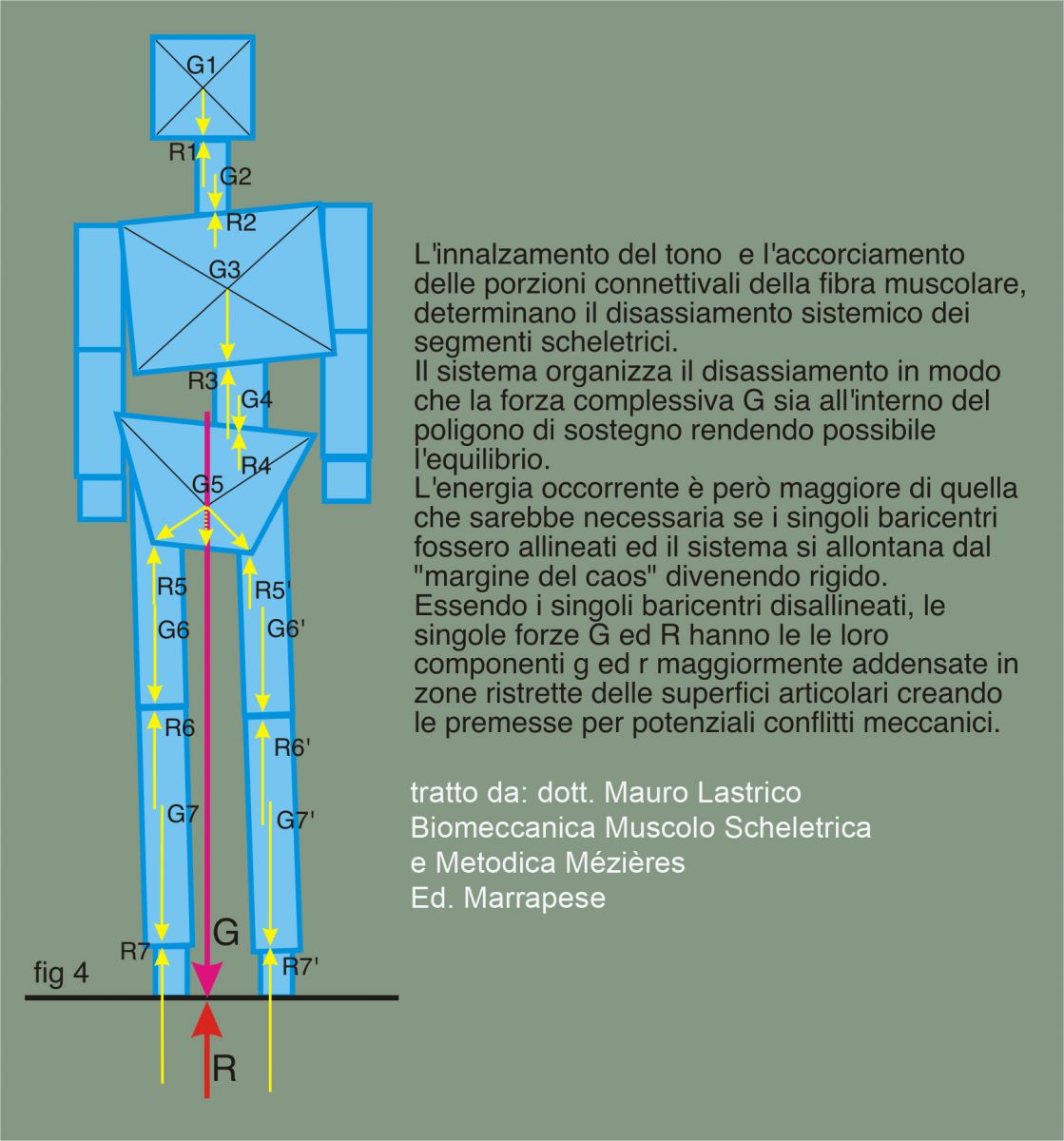
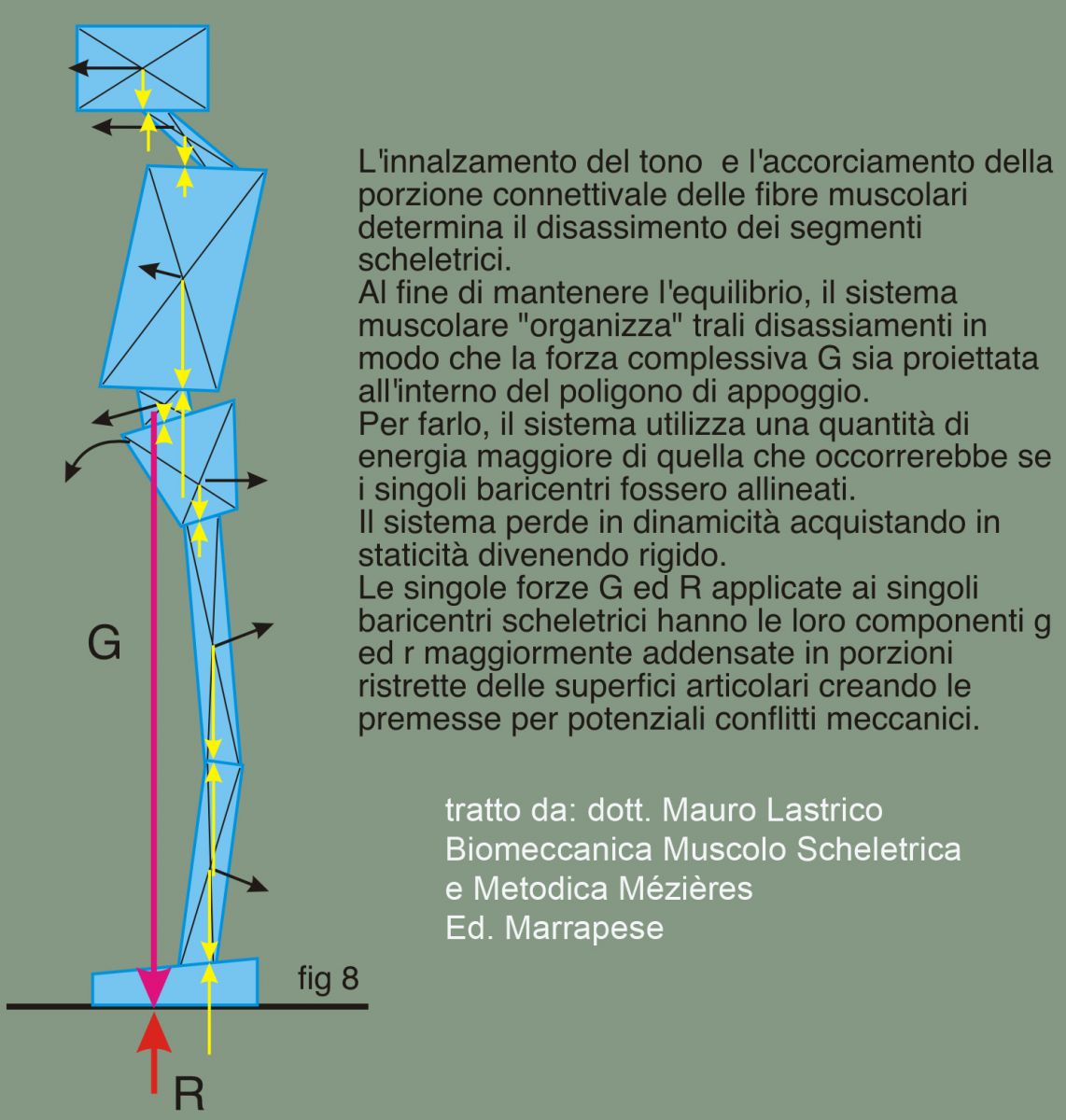
In figure below, muscular system misaligns body segments.
Couple G and R are inside support polygon and equilibrium is possible though at price of skeletal district misalignment. Prolonged alteration of physiological articular sequence may cause compressive articular conflicts.
Other problems arise from components g and r which concentrate in small surfaces instead of distributing over support surfaces.
Muscle tone must increase since displacement of one mass center alters initial position of all mass centers, involving entire muscular system. System is in equilibrium but loses dynamism and gains rigidity.
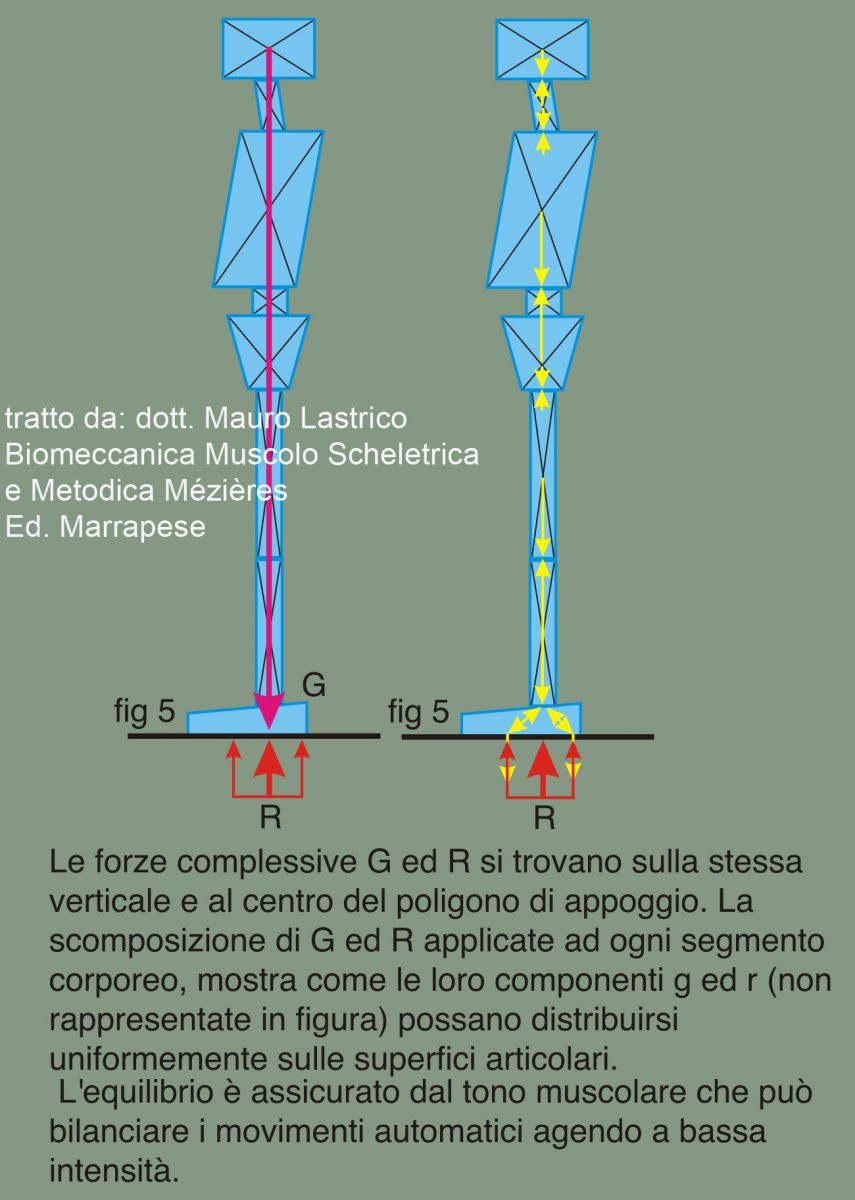
Using similar body geometrization on sagittal plane shows how individual mass centers form overall resultant G on vertical of resultant joint reaction R. Reaction passes through apex of medial plantar arch while actual joint reactions apply to forefoot and hindfoot leaving toes free. Components g and r distribute evenly on skeletal support surfaces minimizing compressive moments.
Muscular action may act minimally to verticalize G and R compensating automatic body movements.
Figures show anterior or posterior projection of force G relative to support polygon; reaction R applies at polygon front or rear edge. This causes force moment M given by G and R times distance "d". To prevent balance loss, muscular system must activate strongly.
Example of muscular system "strategy" to bring force G inside support polygon: all skeletal elements project anteriorly or posteriorly. Here, G passes before medial plantar arch apex, so reaction R applies more to forefoot (baropodometric exam would show anterior loading). Skeletal segment displacement occurs by muscle action and since no muscle can self-lengthen, muscle action compresses. Prolonged compression affects connective fiber causing permanent shortening.
Components g and r concentrate on small surfaces creating conditions for structural lesions.
With aligned barycenters, moving from static to dynamic phase requires minimal muscle activation creating gravity/ground reaction couple favoring walking. Elements of staticity and dynamicity are optimally organized, system at "edge of chaos" (4th complex systems feature). It can use small energy amounts to transition between states.
If muscular shortenings exist, body barycenters misalign and basal muscle force for balance increases.
Basal tone increase causes connective portion shortening, creating a self-feeding circuit: misaligned barycenters force basal tone increase causing muscular shortening further misaligning barycenters.

This modifies vertebral sinusoid and overall body barycenter lowers. Moving from static to dynamic phase requires more muscle action: system loses dynamism but gains stability, moving away from "margins of chaos" becoming rigid.
Conclusions
The neuromuscular, psychosomatic, and biomechanical systems all rely on the muscular system to achieve their respective objectives. Moreover, in accordance with the fundamental properties of complex systems, they are interactive and interdependent: regardless of which system is primarily involved in the imbalance, the others must implement adaptive strategies to preserve function as effectively as possible. In this sense, they behave as an integrated system.
The involvement of the muscular system manifests through an increase in basal tone and both segmental and systemic muscular contraction.
When such contraction and/or increased basal tone persist over time, the connective portion of the muscle fiber becomes involved, leading to residual shortening. This in turn causes a misalignment in the physiological joint sequencing, which then triggers further muscular contraction and elevated tone—thus creating a self-perpetuating loop.