

Considerations on the Iliopsoas Muscle
Dr. Giuliano Chiri
Considerations on the Iliopsoas Muscle
Chiri Giuliano, Ft. D. O.
Abstract
This highlights the correlation between the state of spasm-shortening-fibrosis of the psoas, irritation of nerve structures (femoral nerve, …) and osteopathic dysfunctions of visceral organs (kidney, gastroesophageal junction, colon). Some anatomical references to the insertions of the psoas muscle and its relationships with muscular, fascial, skeletal, nervous, visceral structures are integrated for the reader's use. INSERTIONS
The iliopsoas muscle is formed by two distinct muscles at their origin
1. Psoas major: originates from the lateral surface of the body of the last thoracic vertebra and from L1;L2; L3; L4. Some fibers insert on the intervertebral discs and at the base of the transverse processes of the last four lumbar vertebrae. It runs downward and laterally outward, crossing the lumbar and iliac area, passes inferiorly (below) to the inguinal ligament and inserts on the trochanter, passing in front of the hip joint.
2. Iliacus: fan-shaped and originates from the inner lip of the iliac crest, throughout the iliac fossa and its circumference, on the ilio-lumbar ligaments and at the base of the sacrum (lateral portion of the sacral wing). It inserts together with the tendon of the psoas major muscle.
FIG 1 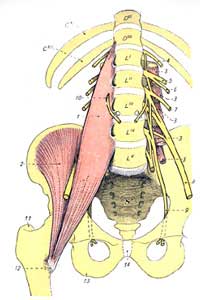
Innervation
The iliopsoas muscle receives its innervation from muscular branches of the lumbar plexus and the femoral nerve with roots L1-L4. ANATOMICAL RELATIONSHIPS
The psoas major has relationships with
• the medial diaphragmatic arch,
• the kidney,
• the ureter,
• the renal vessels,
• the ascending colon on the right,
• the descending colon on the left.
• It houses the femoral nerve.
The iliacus muscle has relationships with
• the cecum,
• the appendix on the right,
• and the iliac colon on the left.
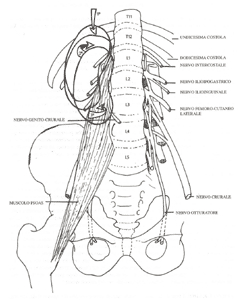
FIG.2

Relationships with the Iliac Fascia
In front of the iliopsoas muscle extends one of the most important fascias: the lumbosacral fascia.
• This fascia transversely occupies the entire width of the iliac fossa and extends in height from the superior insertion of the psoas major muscle to the trochanteric insertion of the same muscle. In summary, it inserts all around the iliopsoas muscle.
• The iliac fascia has relationships with: all the lumbar vertebrae, the base of the sacrum, the superior base of the small pelvis, the aponeurosis of the quadratus lumborum muscle, the ilio-lumbar ligament and the iliac crest (medial lip), with the psoas major muscle, at the level of the fibrous arch of the psoas major (in turn related to the diaphragm), with the inguinal ligament, below the inguinal ligament (boundary between the pelvis and the thigh) the iliac fascia accompanies the extra-pelvic portion of the iliopsoas muscle.
The iliac fascia continues into the thigh.
• With the femoral fascia that descends with the sartorius muscle.
• With the fascia of the pectineus muscle
The condition of suffering or pathologies affecting the iliopsoas muscle can cause various clinical signs, symptoms near the same district but also located at a distance. Besides the evaluation of the musculoskeletal components and the well-known interactions between psoas, lumbar spine and diaphragm muscle, the osteopathic contribution seems interesting as it broadens the perspective regarding the iliopsoas, considering the interaction with adjacent structures and in particular the possible
• involvement of nerve structures, such as:
the lateral femoral cutaneous nerve
the genitofemoral nerve
the obturator nerve
the femoral nerve, with corresponding dermatome involvement.
• involvement of the abdominal sympathetic chain, which rests on the psoas aponeurosis. The iliopsoas can influence the sympathetic system, as well as being affected by any influence having a tonic sympathetic component.
The symptomatology is explained both by the possibility of direct contact between the ganglia of the lateral vertebral chain and the psoas, and by the mediation of the orthosympathetic arterial vascular system
• involvement with the visceral system
Kidneys: the retrorenal fascia covers the quadratus lumborum muscle and subsequently the psoas, attaching itself at the vertebral level
Ureter, liver, duodenum, ascending colon, cecum, descending colon and vermiform appendix have direct relationships with the iliac fascia or with the iliopsoas muscle.
FIG.3
Regarding interactions with the visceral system
The psoas muscle and sacroiliac joints are subject to frequent fixations, especially because this muscle is innervated by lumbar nerve plexuses that also serve most of the abdominal organs.
According to Barral (Visceral Manipulation, 1998), the psoas muscle often undergoes spasm in patients suffering from gastro-esophageal problems, partly because its ligaments exchange fibers with the diaphragm, and also because the sympathetic nerves that cross it may suffer irritation.
Also according to Barral, the condition of renal ptosis may be accompanied by involvement of the femoral nerve. From the dysfunction perspective, the psoas muscle acts as a track along which the kidney moves caudally. In this case, a clinical picture can occur described as hypersensitivity of the ipsilateral thigh accompanied by knee pain without previous trauma in that area. The internal capsular pain increases when bending the joint, so that kneeling or squatting are poorly tolerated positions.
The knee pain leads to a spasm that tends to rotate the lower leg externally, with a change in the axis of the lower limb, causing joint pain manifesting in the ankle and foot and mechanical problems, even if they are of visceral origin (Barral, op cit).
Bibliography
1) Testut Latarjet– "Human Anatomy" , UTET To 1972
2) J.P. Barral – "Visceral Manipulation" (vol 1 and 2) , Castello Editore- Mi 1998
Sobotta – Atlas of anatomy.