Biomechanics of the Spine in the Sagittal Plane
Dr. Mauro Lastrico
Spinal Biomechanics: Sagittal Plane
Dr. Mauro Lastrico, Physiotherapist.
Excerpt from:
"Musculoskeletal Biomechanics and Mézières Method"
Author: Dr. Mauro Lastrico
Marrapese Publisher
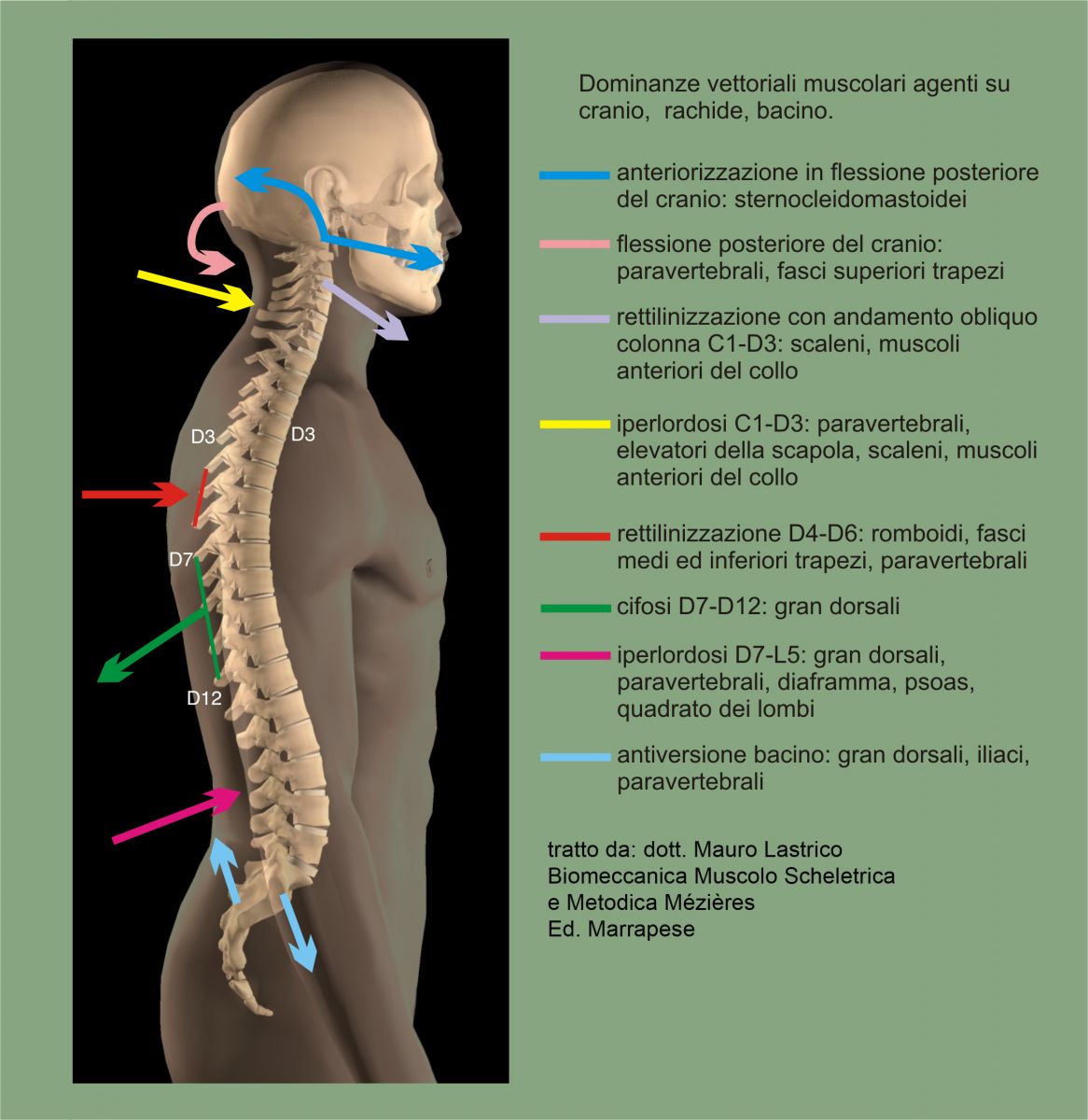
By observing the anatomical arrangement of muscles directly influencing the spine, pelvis, and skull, one can complement the anatomical division of the spine with a myofunctional musculoskeletal division distinguished into:
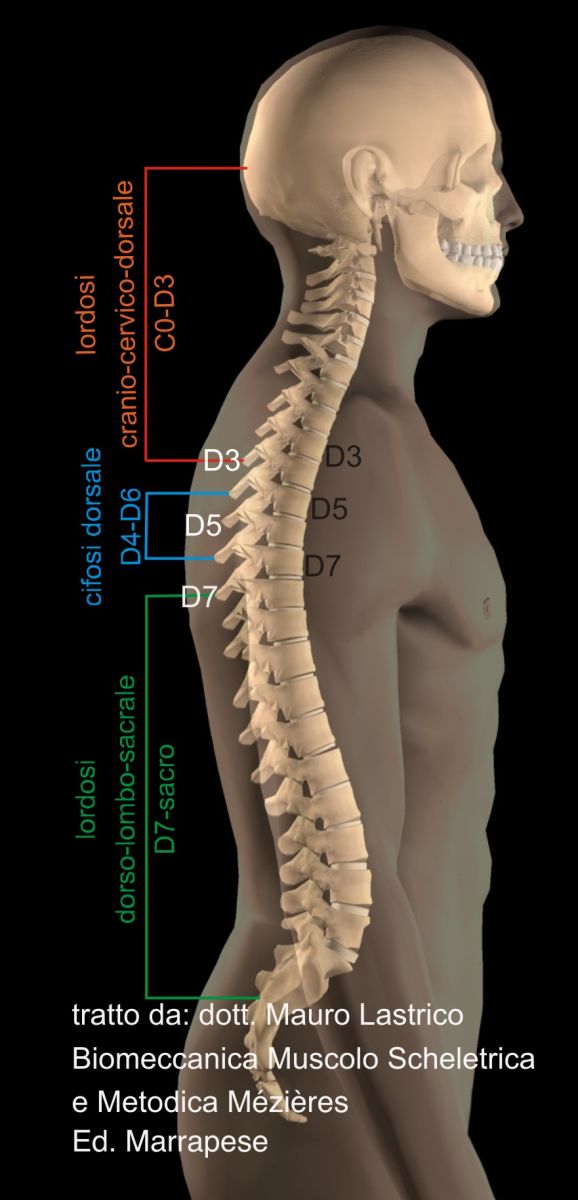
- cranio-cervico-dorsal lordosis extending from the skull to the spinous process of D3
- dorsal kyphosis extending from the spinous process of D4 to that of D6
- dorso-lumbo-sacral lordosis extending from the spinous process of D7 to the sacrum.
Cranio-cervico-dorsal lordosis
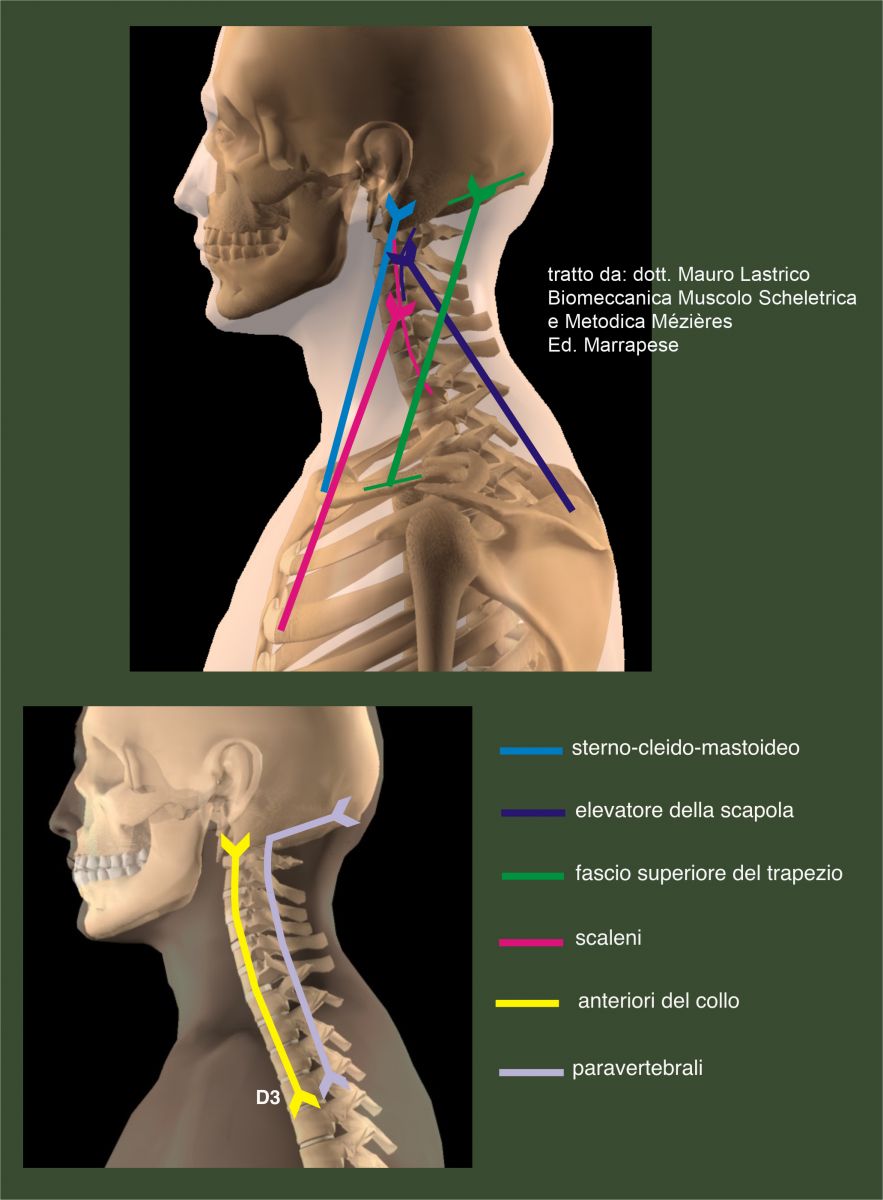
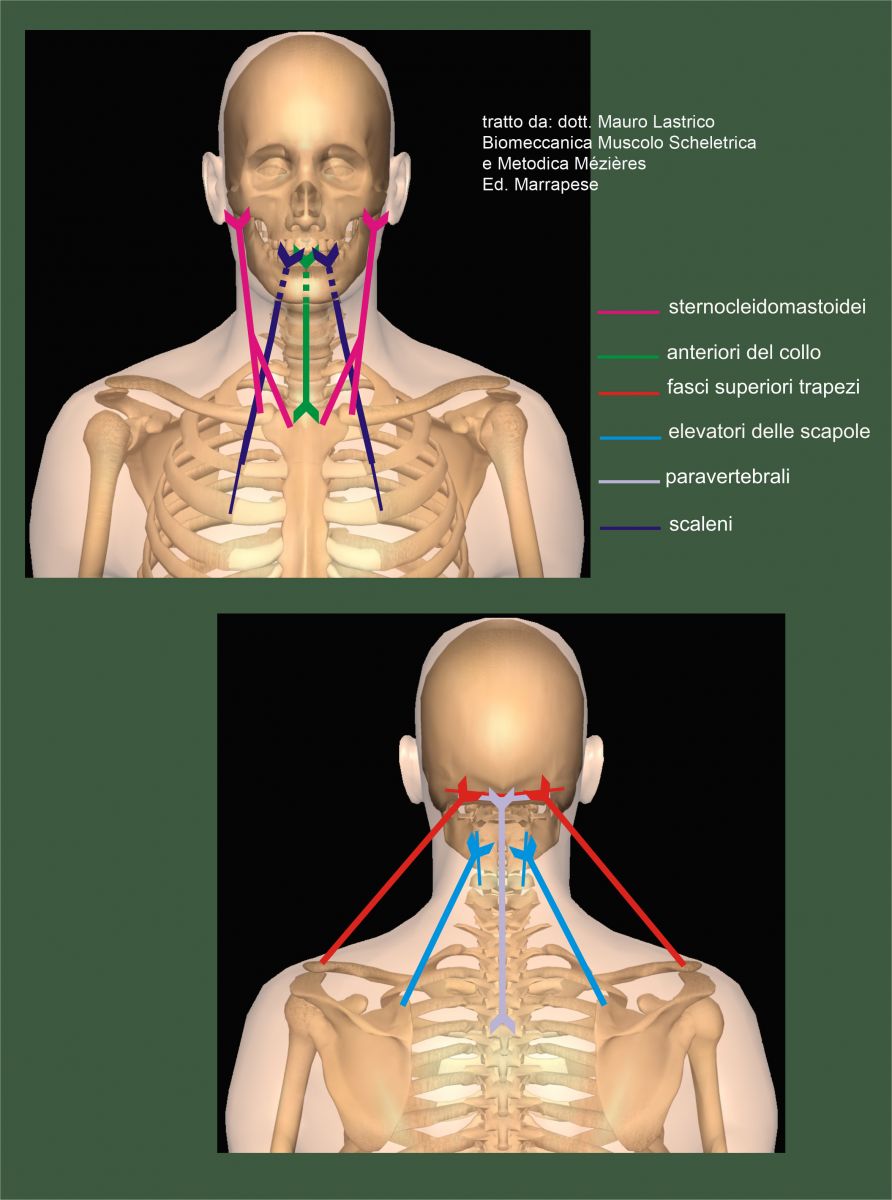
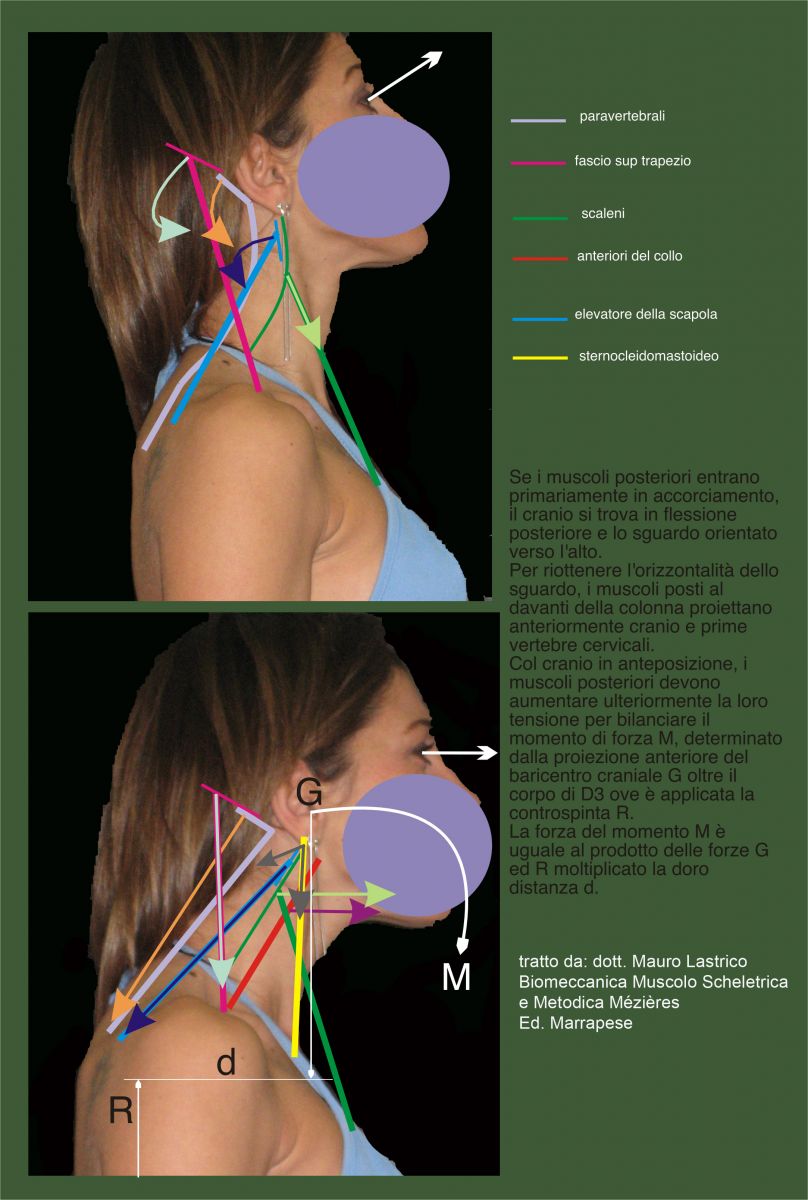
It is the only spinal tract where muscles with dual insertion on the spine are present both anteriorly (anterior neck muscles) and posteriorly (paravertebrals). The muscular support to the prolongation up to D3 of the cervical lordosis is given precisely by the muscles in front of the cervical spine inserting up to D3: rectus capitis anterior, longus capitis, longus colli.
Anteriorly also the scalenes and sternocleidomastoids.
Posteriorly the paravertebrals, levator scapulae, and upper fibers of trapezius.
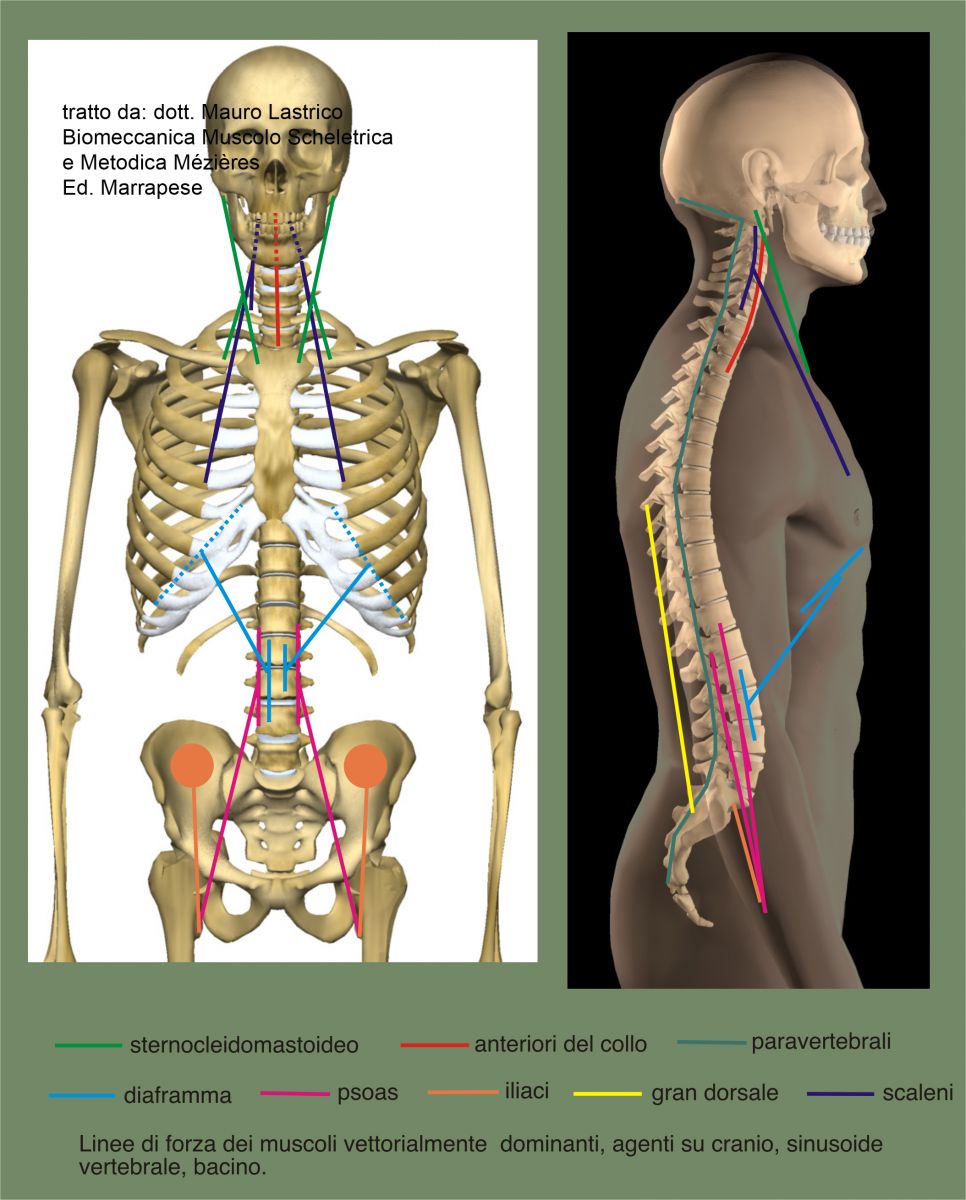
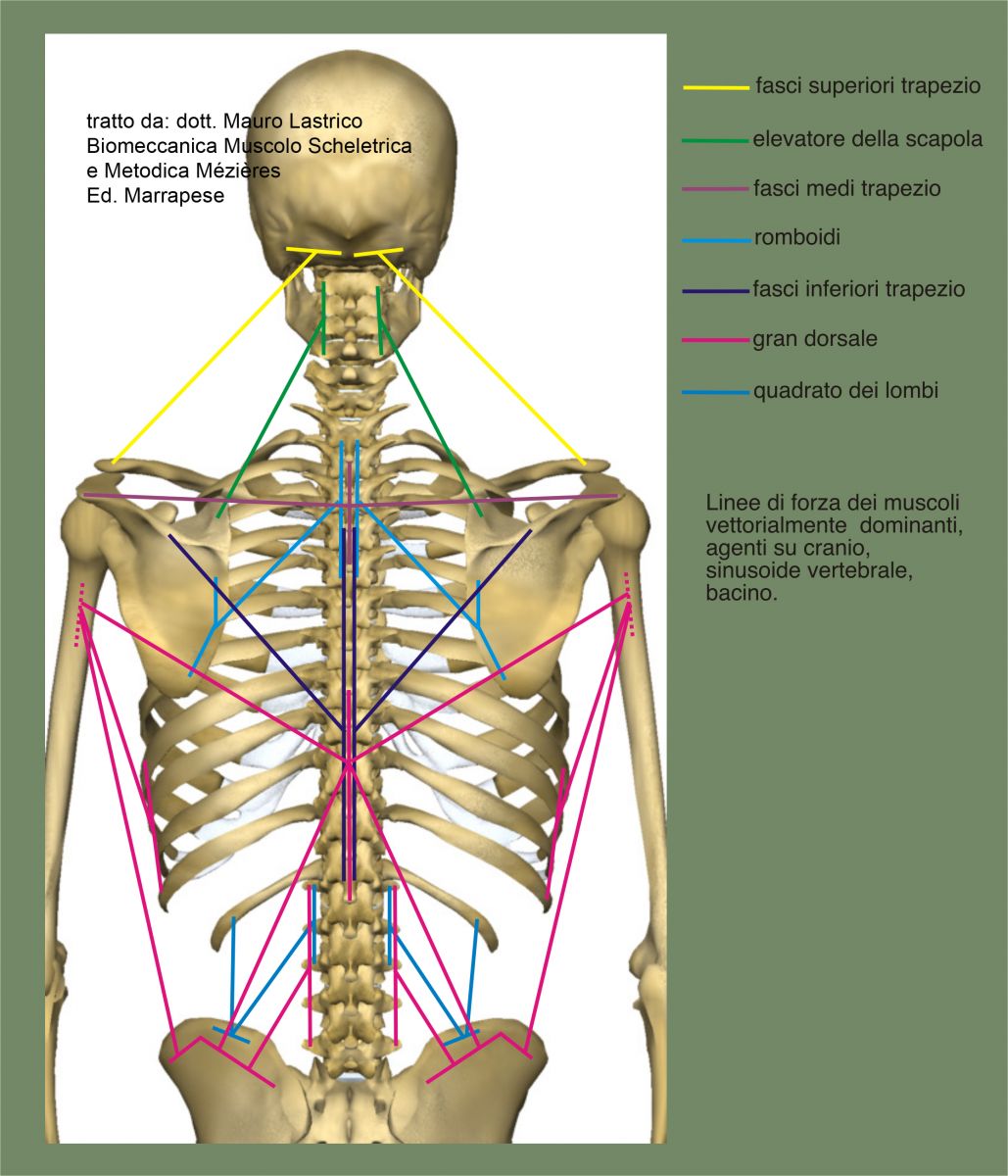
In the following figures, the force lines of the individual muscles are represented, considering the cranial and vertebral insertions as mobile points.
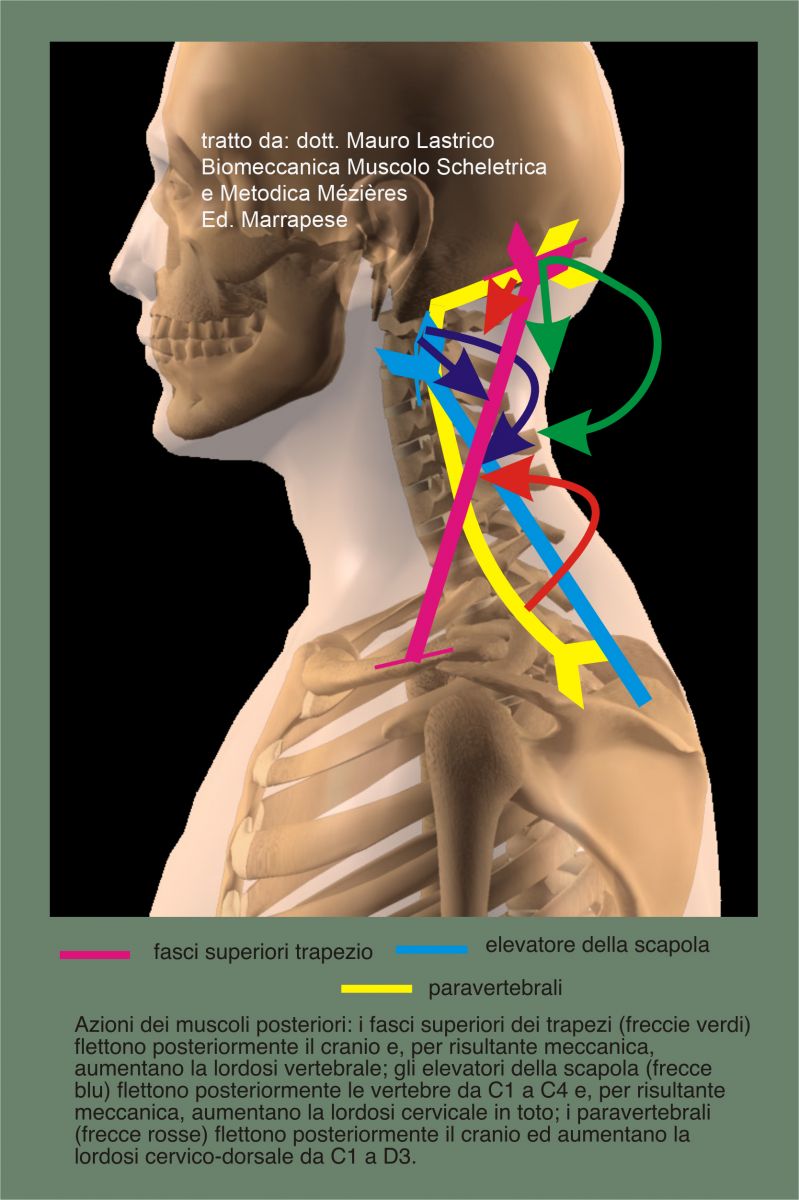
Posterior muscles:
Increased basal tone and subsequent shortening cause:
- posterior flexion of the skull due to the direct action of the paravertebrals and upper trapezius fibers and indirectly due to the levator scapulae
- increased cervical lordosis due to the direct action of the paravertebrals and levator scapulae and indirectly due to the upper trapezius fibers
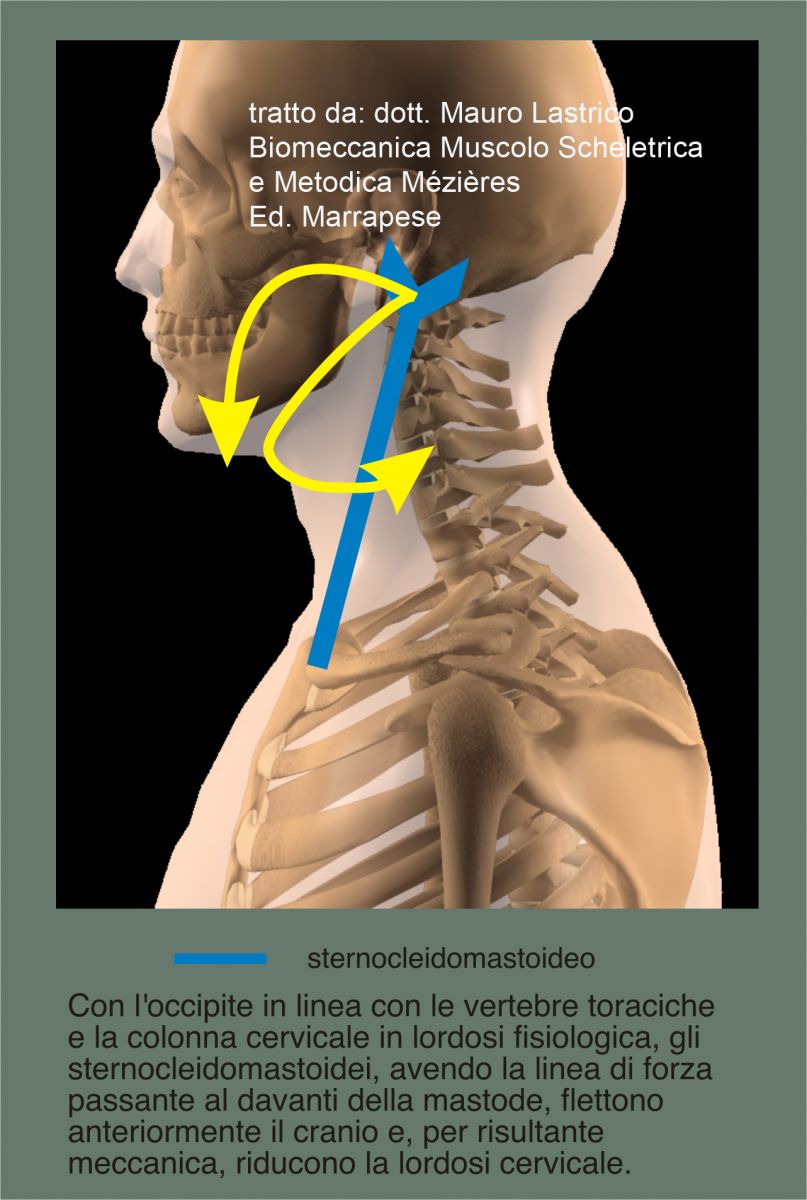
Anterior muscles:
Their involvement creates different patterns depending on whether the skull maintains or not its alignment with the apex of the physiological kyphosis
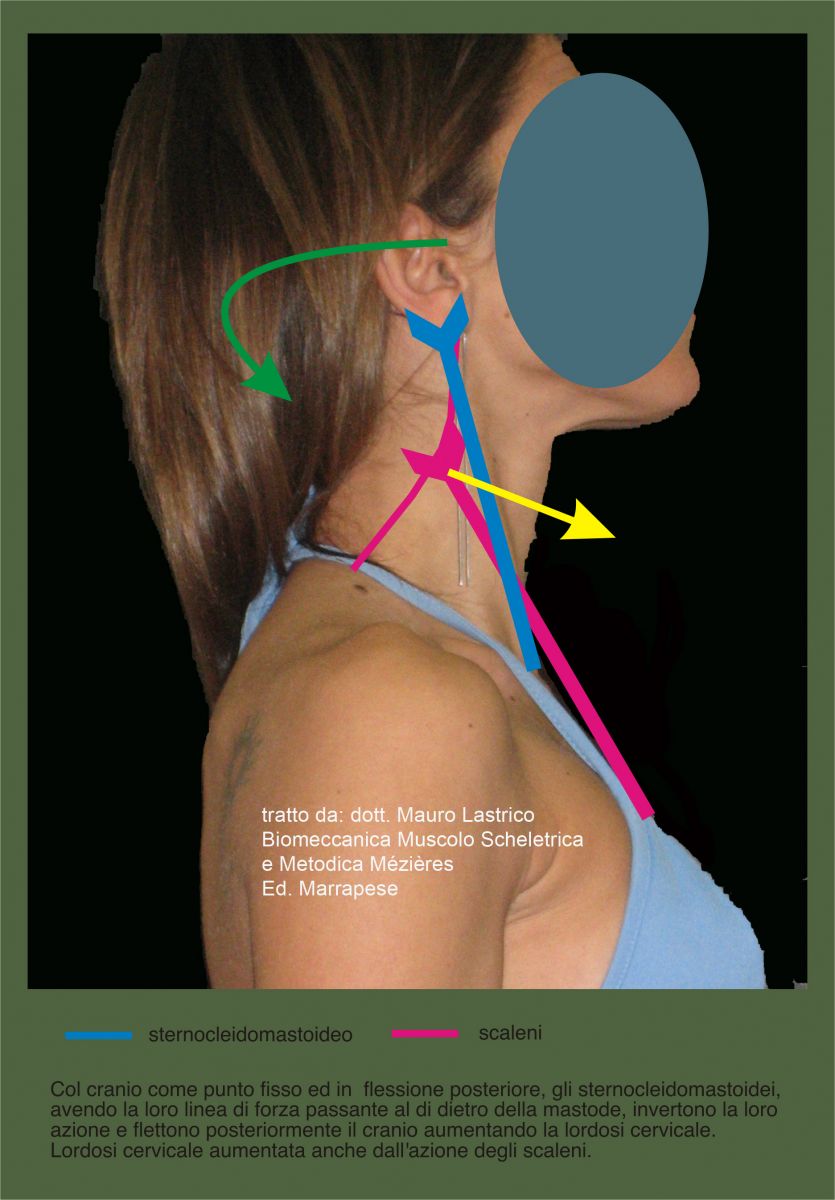
- with the occiput on the same vertical line as the dorsal kyphosis and the cervical spine in physiological lordosis: the sternocleidomastoids, in their bilateral action, flex the skull anteriorly causing a mechanical result of lordosis reduction;
However, if the skull position is in posterior flexion, the force line of the sternocleidomastoids passes behind the mastoid, causing inversion of action. They will flex the skull posteriorly contributing to lordosis increase together with the scalenes.
The anterior neck muscles (rectus capitis anterior, longus capitis, and longus colli), when the spine is in physiological lordosis and the occiput aligned with thoracic vertebrae, have a force line passing anteriorly to the sagittal midline dividing the vertebrae; in this case their action is to straighten the cervical tract.

If the spine is hyperlordotic, the force line passes posteriorly to the midline and in this case the action becomes opposite: the anterior neck muscles increase lordosis.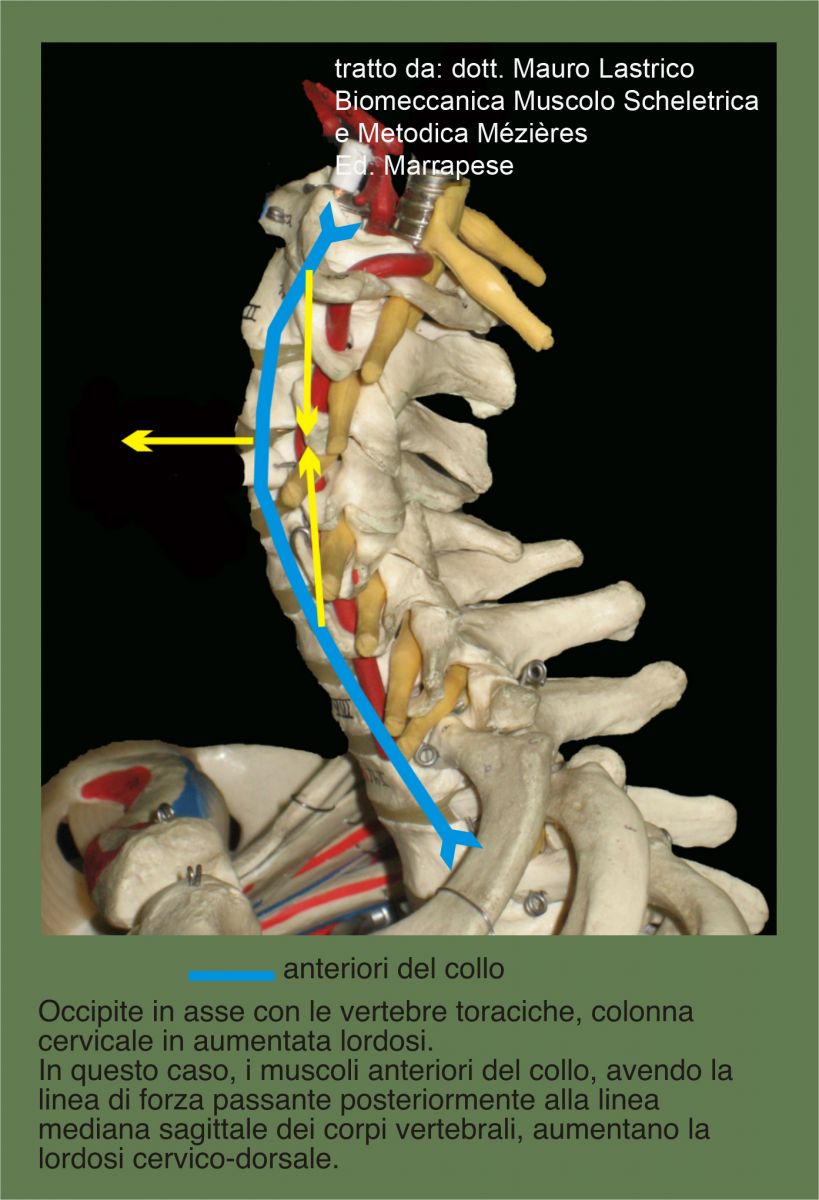
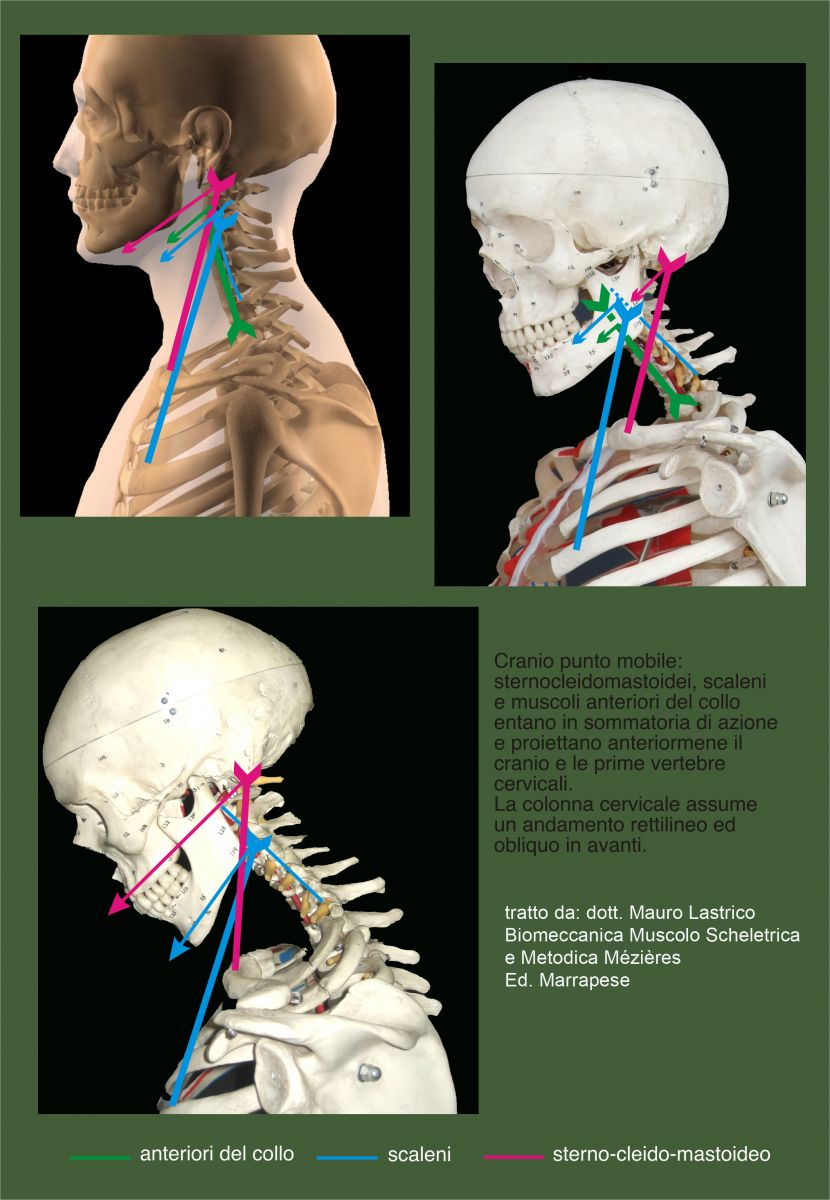
- With the skull as the mobile point: for strategic needs of the complex musculoskeletal system, sternocleidomastoids, scalenes and anterior neck muscles act synergistically producing anterior projection of the head straightening the cervical spine obliquely.
The recovery of gaze orientation occurs through contraction of the posterior paravertebrals and upper trapezius fibers which flex the skull posteriorly.
Skull
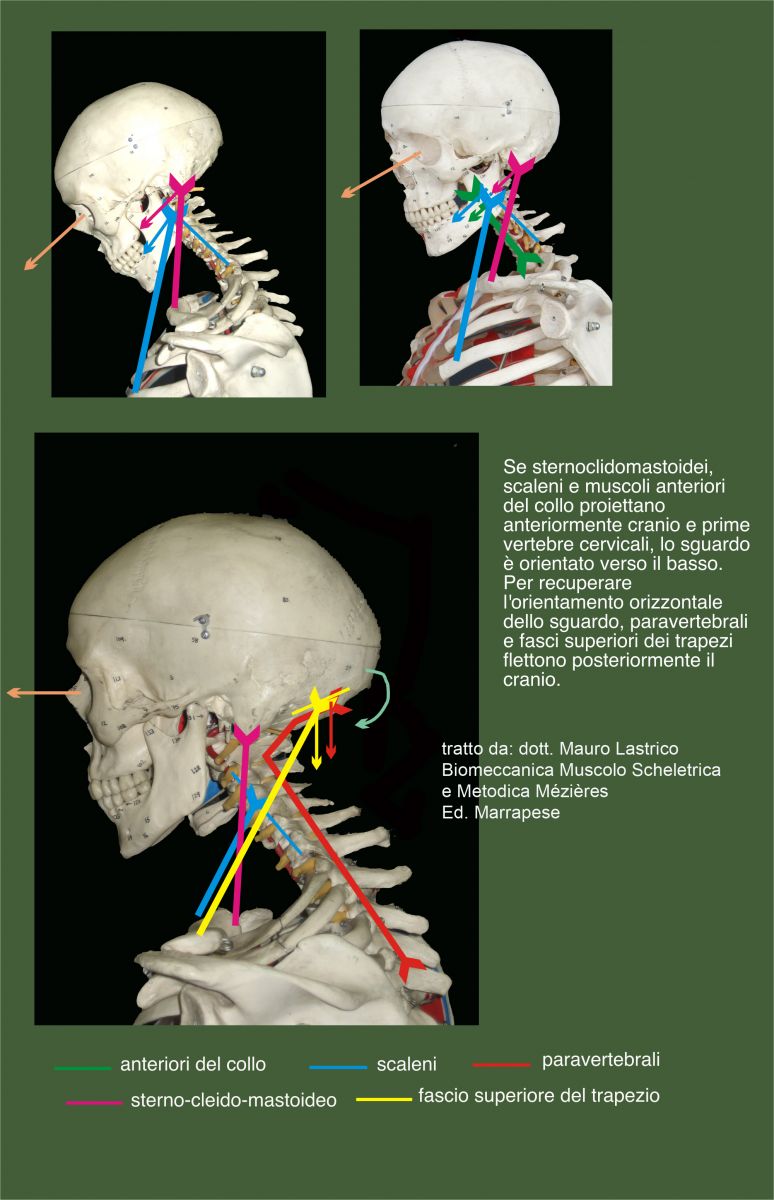
Postural reflexes interact to maintain the skull position well oriented in space, with the eye line as horizontal as possible, involving all cranio-cervico-scapular muscles.
Vectorially, the muscles that increase cervical lordosis, directly or indirectly, are dominant and their shortening also causes posterior flexion of the head interfering with vision.
To recover horizontal eye orientation, the anterior muscles of the cervico-dorsal spine enter excessive tension and, "rolling out" the spine forward, project the skull anteriorly. The sternocleidomastoids directly contribute to this anterior projection.
Horizontal vision is thus restored but the cranial center of mass is no longer aligned with the D3 vertebral body.
Thus, a moment of force M is generated by the product of force G applied to the cranial center of mass and the equal and opposite force R applied to the D3 body multiplied by their distance. This moment of force can be balanced by further tension of the posterior occipital insertion muscles (paravertebrals and upper trapezius fibers) and upper vertebral muscles (levator scapulae).
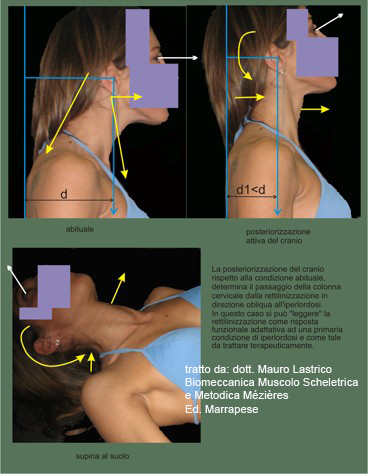
Consequently, in radiographic patterns showing cervical spine straightening, its oblique anterior trajectory may result from contraction and subsequent shortening of anterior muscles that counteract initial cervical hyperlordosis induced by posterior muscle tension.
The straightened and oblique course could also reflect primary involvement of anterior muscles that shift the skull forward with the gaze directed downward. The recovery of horizontal vision will then be guaranteed by the action of the head extensors.
When radiographically the spine appears straight and vertical, being the pattern incompatible with local muscle action, the straightening results from decreased physiological dorsal kyphosis with apex at D5 caused by dorsal paravertebrals and scapular adductors (see next paragraph).
Even when the cervical spine appears straight and oblique, the cause is hyperlordosis: in the attempt to bring the skull onto the vertical of the dorsal kyphosis (passively, actively or supine), the consequent co-contraction of all muscles acting on the cervical spine reveals lordosis increase.
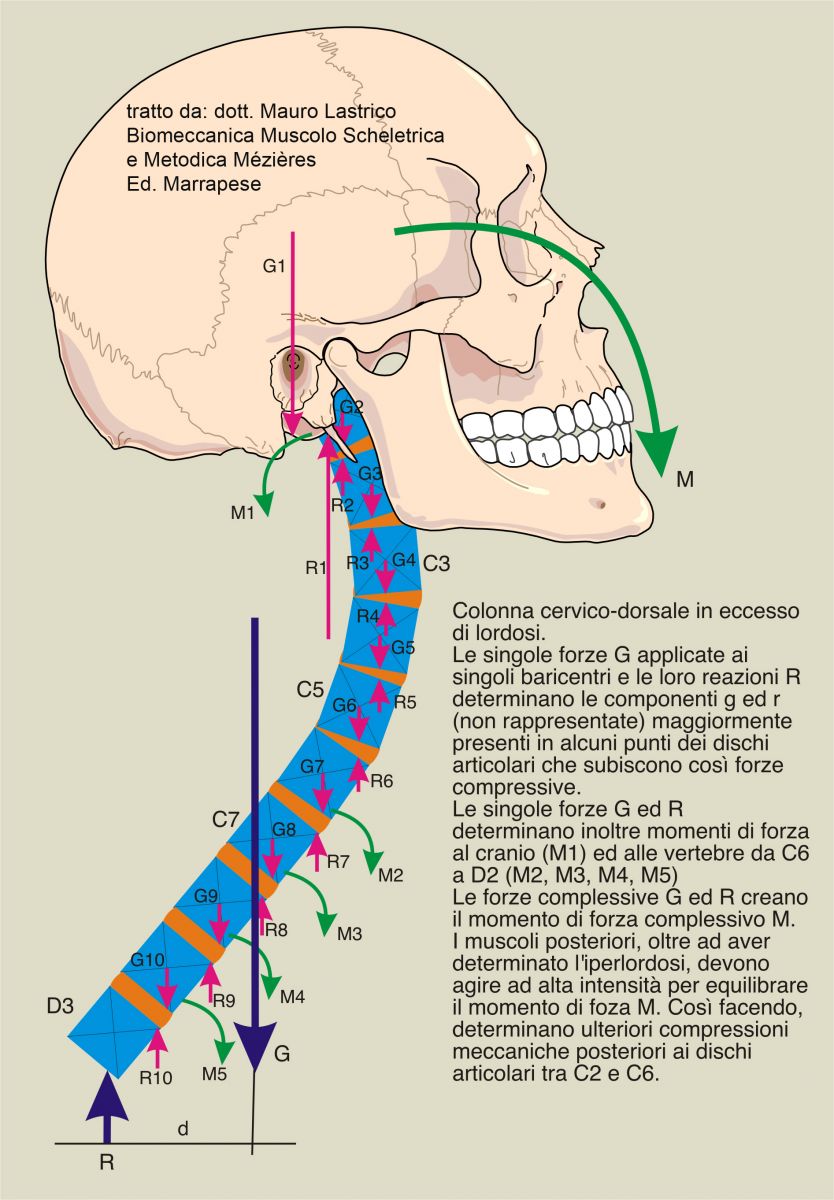
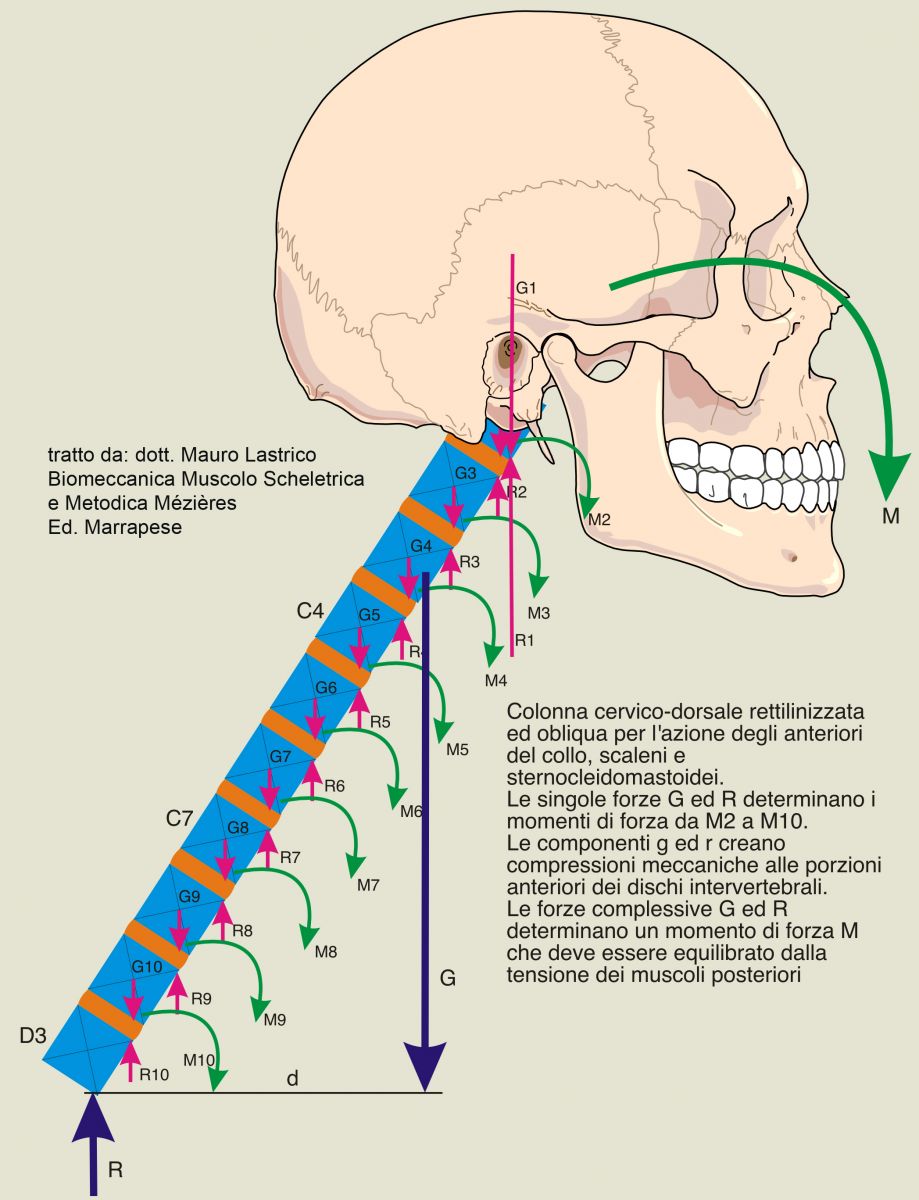
Whether the cervico-dorsal spine shows increased lordosis or straightening with anterior head projection, forces G and reactions R applied to the skull and individual vertebrae cause moments of force and compressions, with their components g and r, on the intervertebral discs.
Overall forces G and R create a resultant moment of force M given by the product of forces G and R multiplied by their distance d. The resultant moment projects the skull towards the floor and, except in lying position, must be balanced by high-intensity activation of posterior muscles: paravertebrals, levator scapulae, upper trapezius fibers.
Dorsal kyphosis
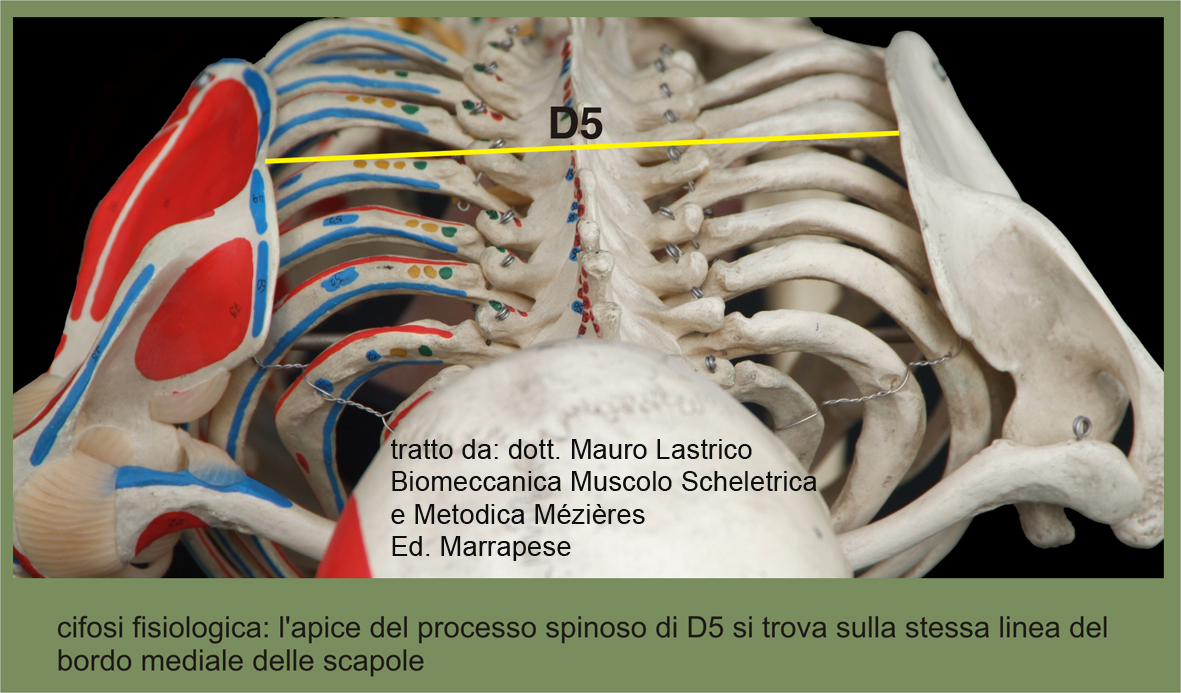
Geometrically, it represents the junction with posterior convexity of the two anterior convexities of the cervico-dorsal and dorso-lumbar lordoses and extends from the spinous processes from D4 to D6, with physiological apex at D5.
When physiological, the apex D5 aligns with the medial margin of the scapulae which lie at the sides of the rib cage.
The muscles having a direct effect on this spinal tract are all posterior (paravertebrals, rhomboids and middle and lower trapezius fibers).
Both the paravertebrals, with longitudinal force lines, and rhomboids and trapezius middle and lower fibers, with oblique force lines, decrease the physiological dorsal kyphosis with apex D5.
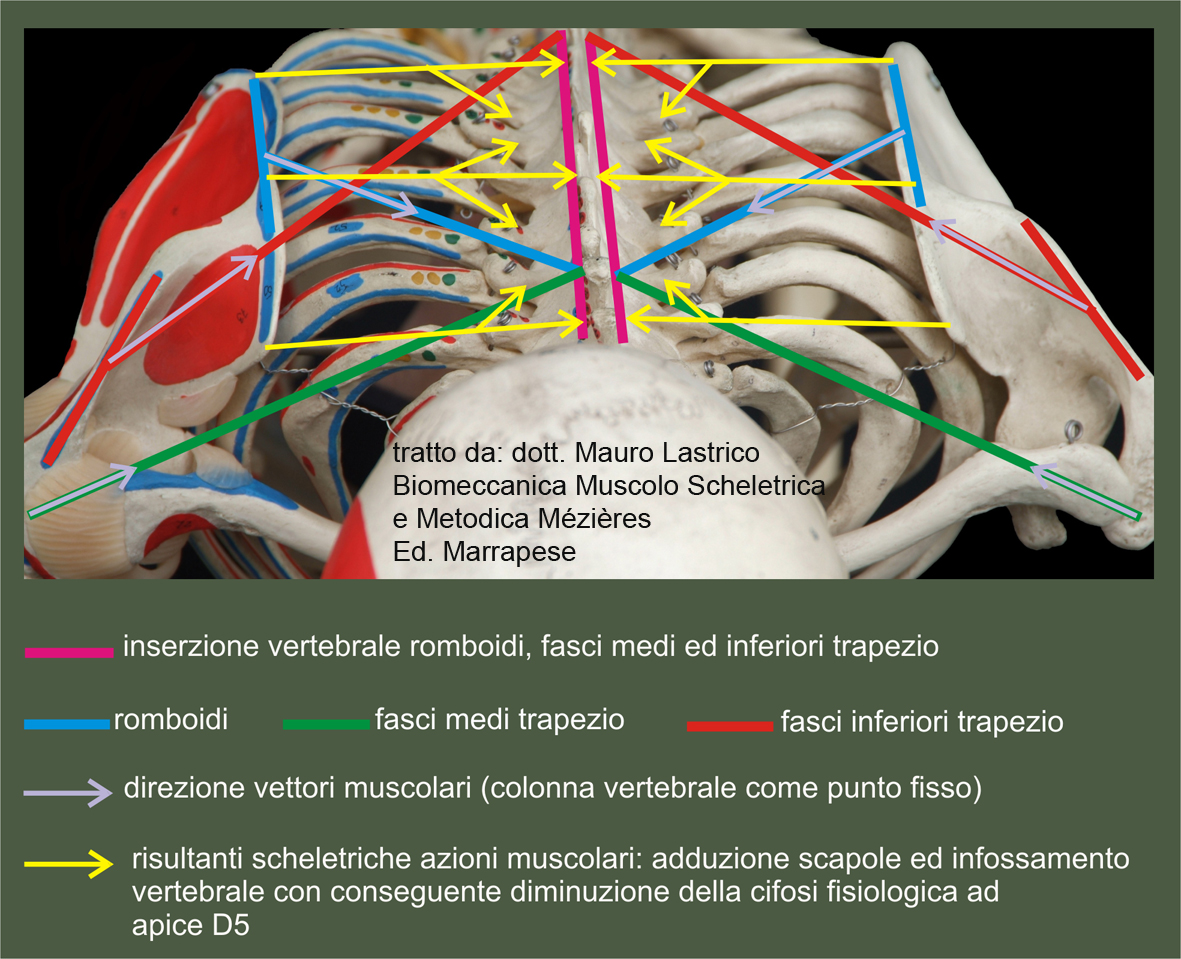
Dorsal hypokyphosis caused by middle and lower trapezius fibers and rhomboids happens due to scapular adduction.
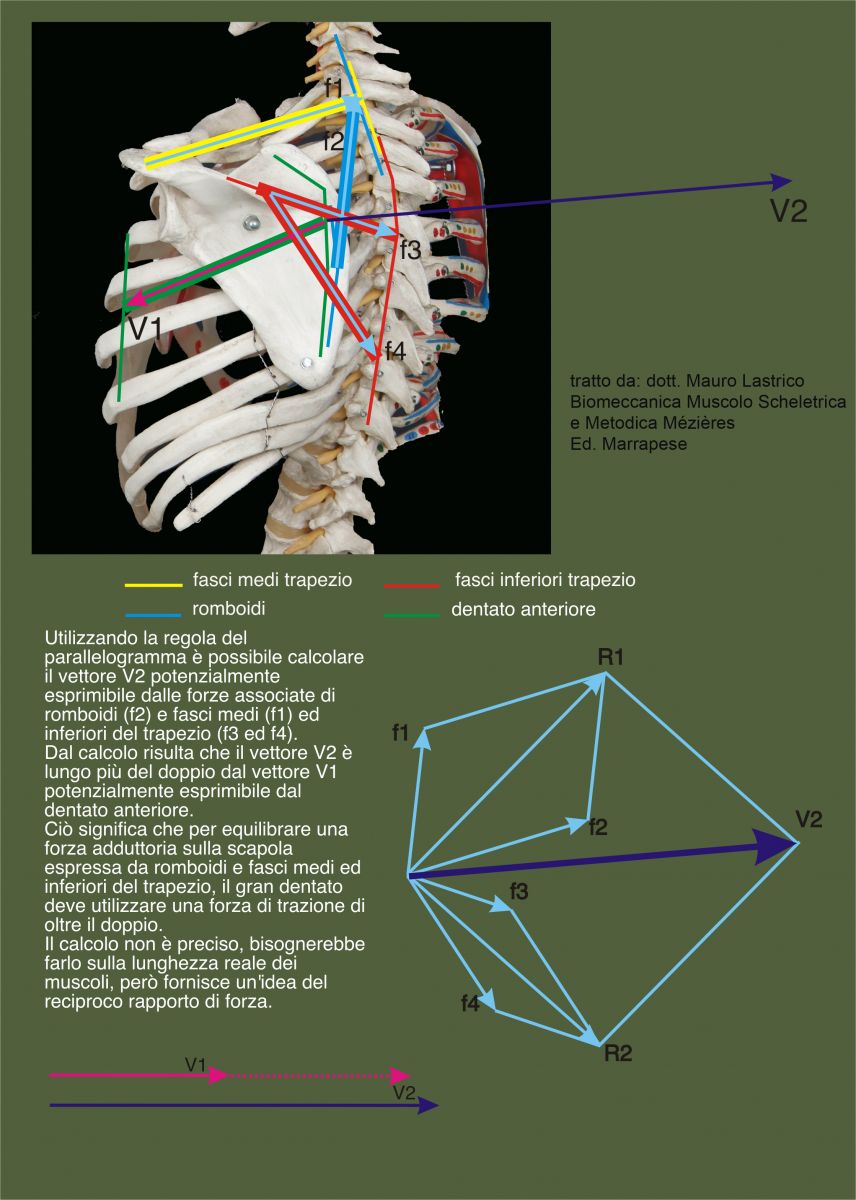
The balance against adduction is ensured by serratus anterior which, however, has a lower vector potential and is subdominant. This vector inferiority becomes even more pronounced considering that the upper trapezius fibers, levator scapulae and latissimus dorsi also participate in scapular adduction.
Consequently, the pulling force of the scapular adductors prevails over the cohesion force of the scapula to the rib cage exerted by the serratus anterior: thus, it is not the scapulae that "protrude", but the spine that "enters".
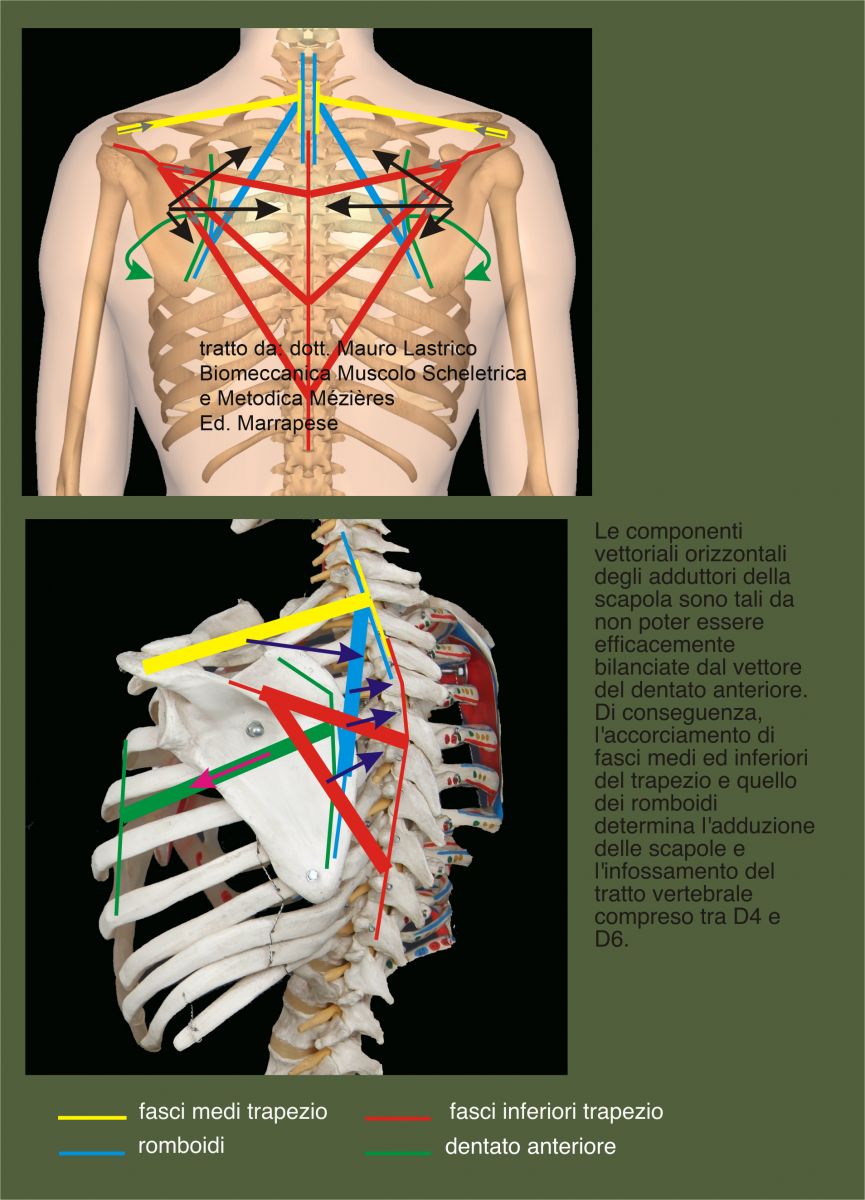
Therefore, the direct muscular action on the infrascapular portion is in straightening (hypokyphosis) of the D4-D6 spinal tract.

In hyperkyphotic patterns, D5 is nonetheless depressed due to scapular adductors and the kyphotic apex is shifted caudally between D7 and D12 due to dorso-lumbar muscles: thus a curve inversion occurs.
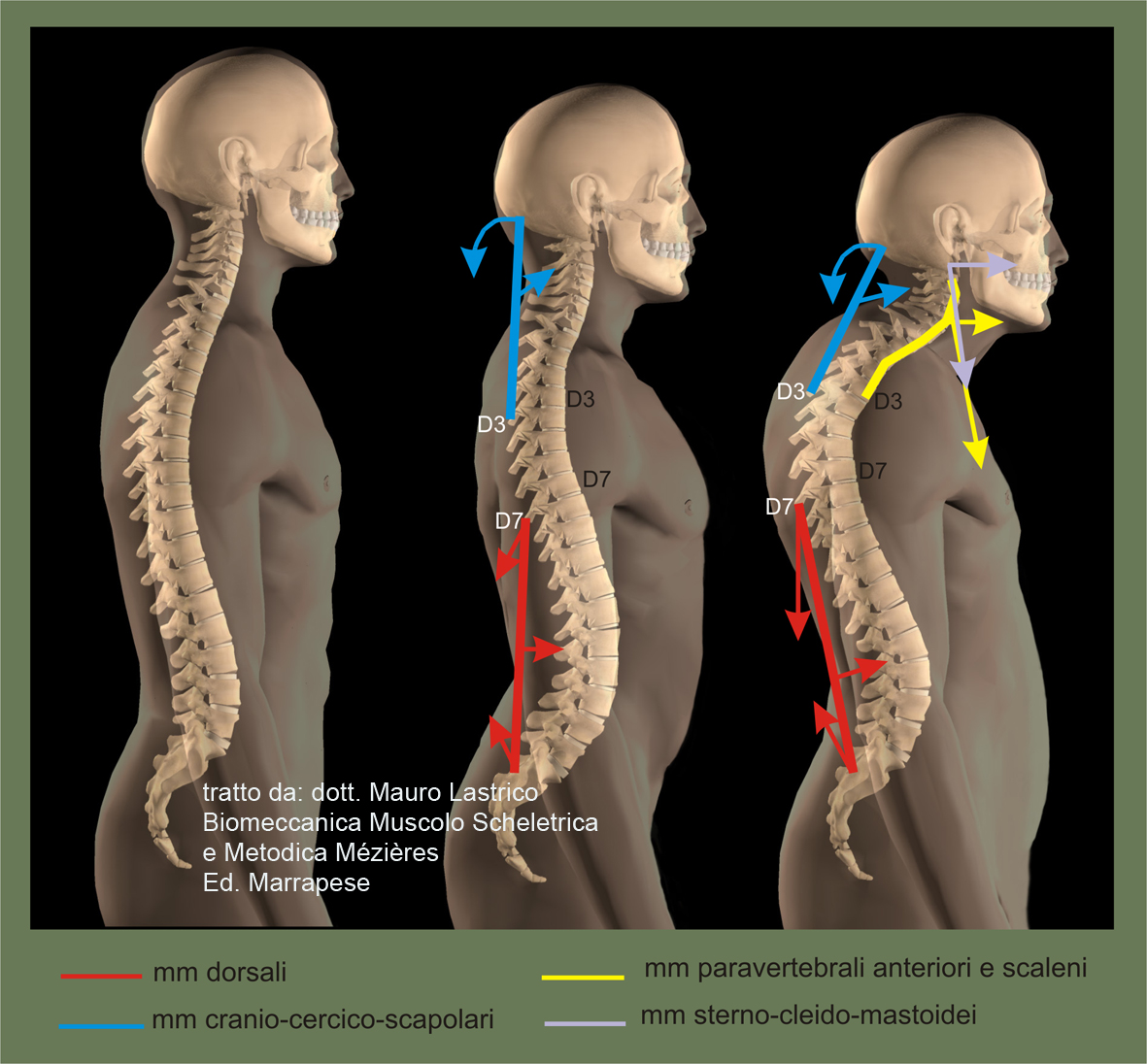
The figure shows the progressive onset of a hyperkyphotic pattern: the cervico-dorsal lordosis muscles increase lordosis and project the head anteriorly to maintain horizontal eye orientation: the physiological kyphotic tract D4-D6 straightens; the dorso-lumbar lordosis muscles increase lordosis and project posteriorly and toward the floor the last dorsal vertebrae which thus become the apex of the kyphosis going into curve inversion.
Dorso-lumbo-sacral lordosis
At lumbar level the dominant vectors with direct insertion on the spine are:
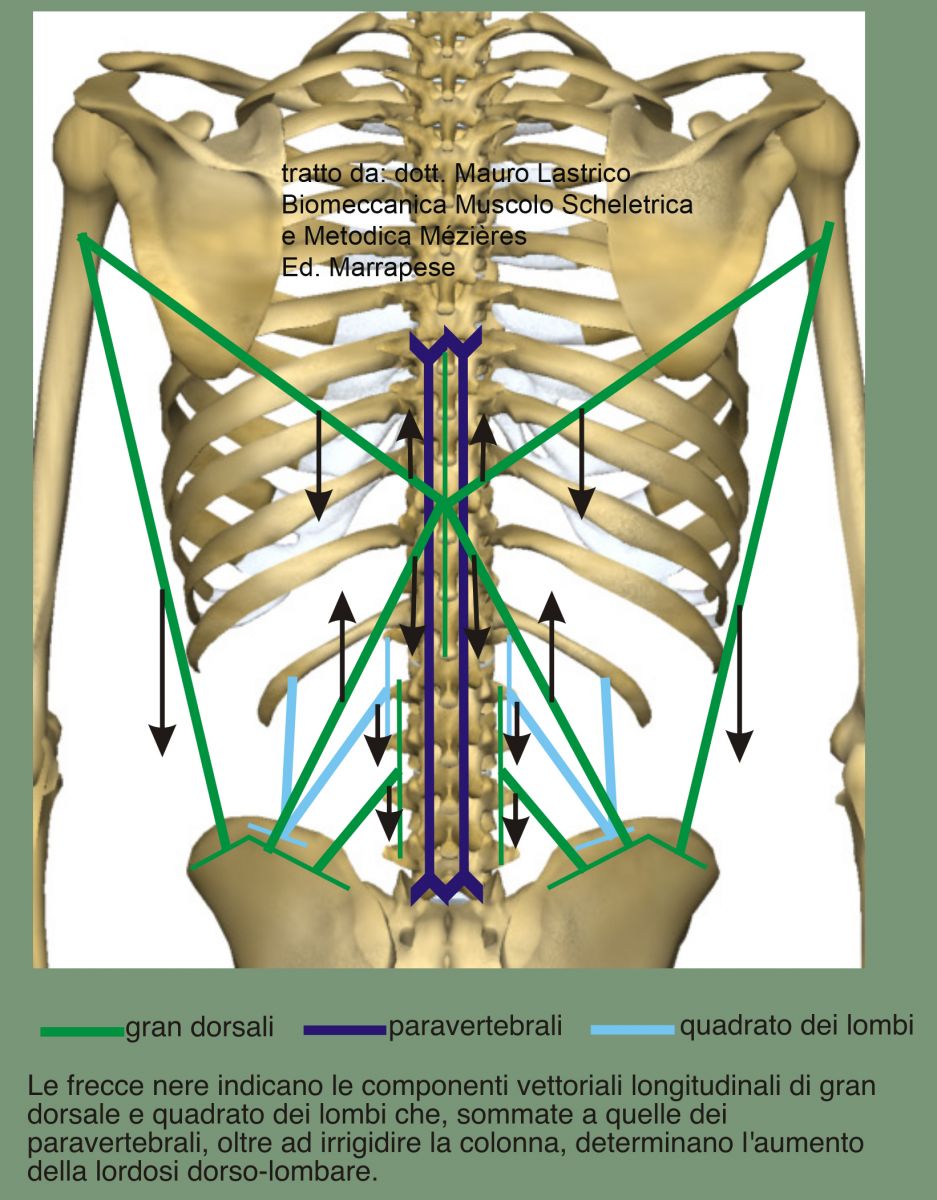
- posteriorly the paravertebrals, quadratus lumborum and latissimus dorsi;
- anteriorly the diaphragm and iliopsoas.
The lumbar lordosis is prolonged by the vertebral insertions of the latissimus dorsi up to D7.
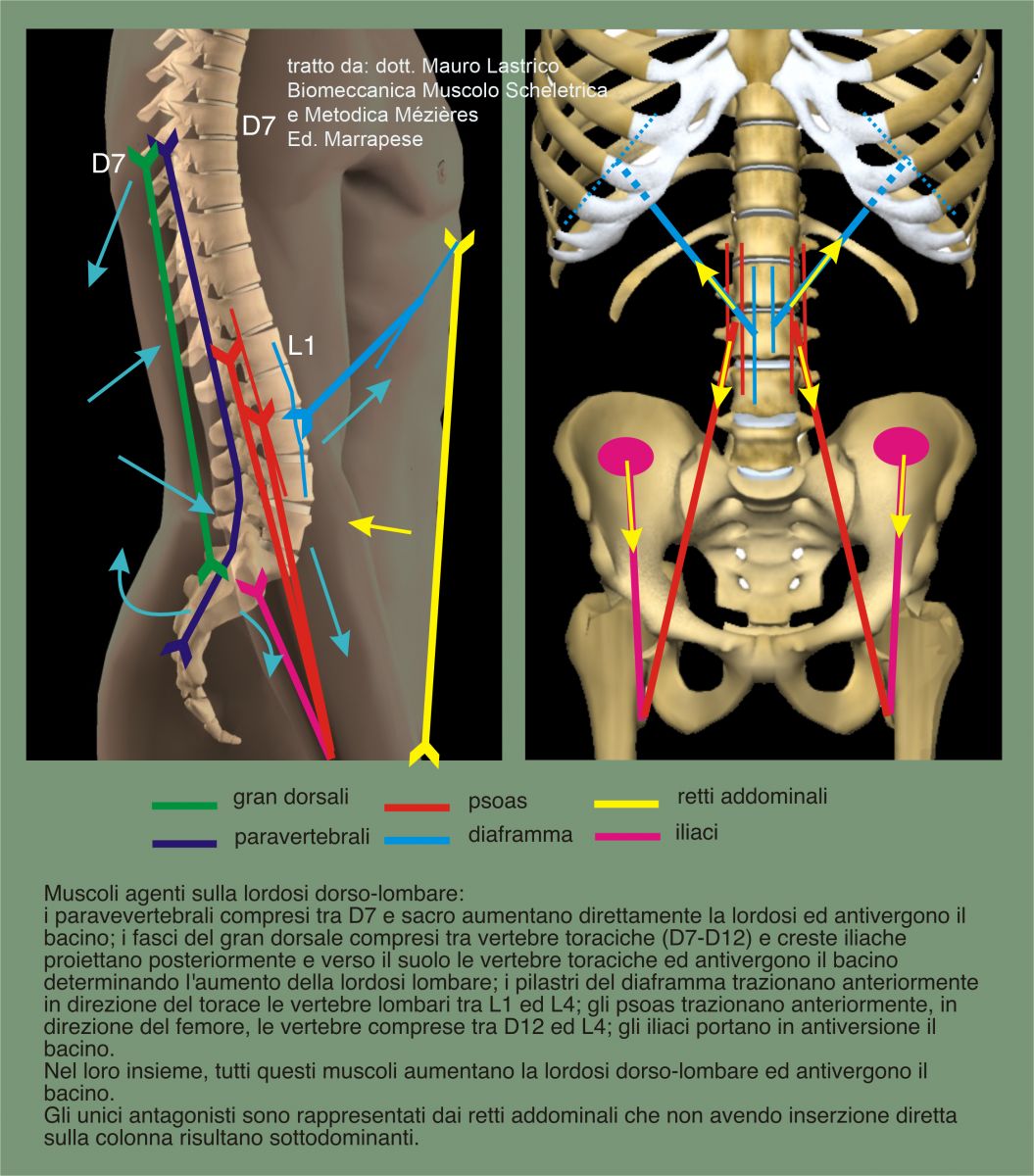
All muscles acting with insertion on the spine are coagonists in increasing dorso-lumbo lordosis. The only antagonists are the recti abdominis which, however, having no direct insertion on the spine and being vectorially inferior, are subdominant. The recti abdominis also have a vertical force line producing horizontally insignificant vectors. The possibility to contain lumbar lordosis is therefore linked to their ability to stiffen the abdominal wall.
All muscles with insertion on the spine instead have force lines both oblique and vertical. This produces vectors that even with a small increase in basal intensity (muscle tone) can modify the curvature of the spine. Oblique force lines have vertical vector components that, adding to those of the paravertebrals, besides increasing lordosis, stiffen the spine.
Moreover, latissimus dorsi, paravertebrals and iliacs create a moment of force that can provoke pelvic anteversion.
The equilibrium is therefore very unstable and even a modest shortening of the muscles acting directly on the spine determines modification of the dorso-lumbar curve projecting it anteriorly.
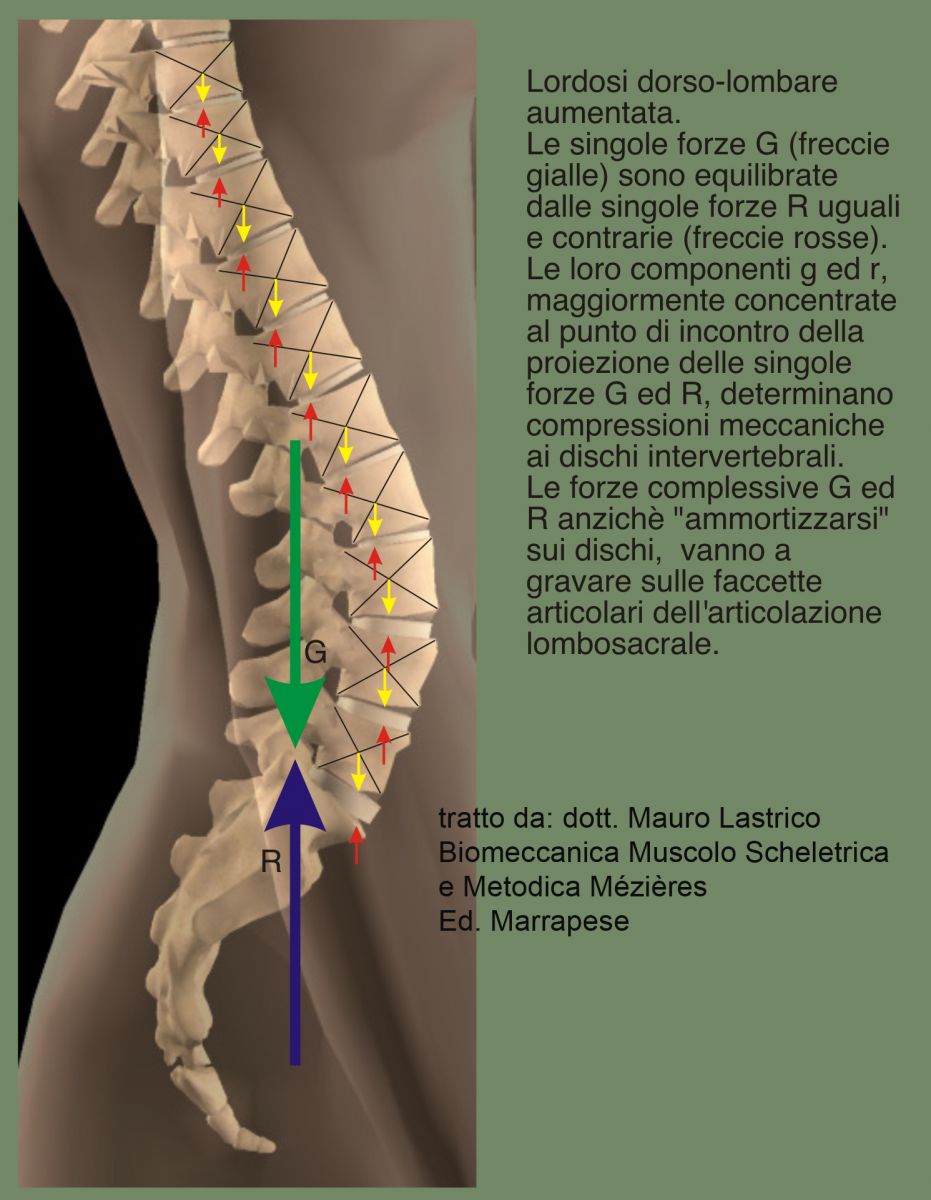
With increased lordosis the single forces G and R applied to each vertebral body determine, with their components g and r, compressions to the intervertebral discs. Overall forces G and R may not meet on a disc, and therefore not be amortized. If their junction occurs on the articular facets of the intervertebral joints, mechanical compressions potentially degenerating into facet fractures may occur.
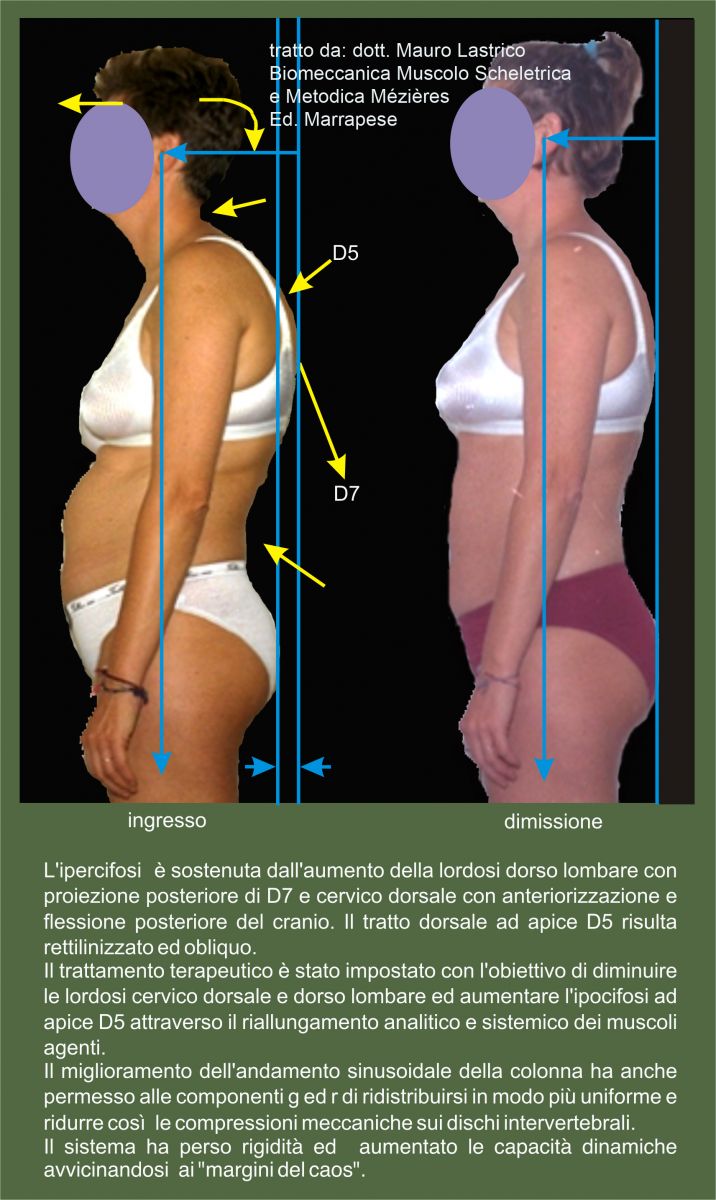
In radiographic patterns showing lumbar straightening, since locally muscles act in opposite directions, verticalization may be the result of pelvic anteversion and/or dorsal kyphosis decrease:
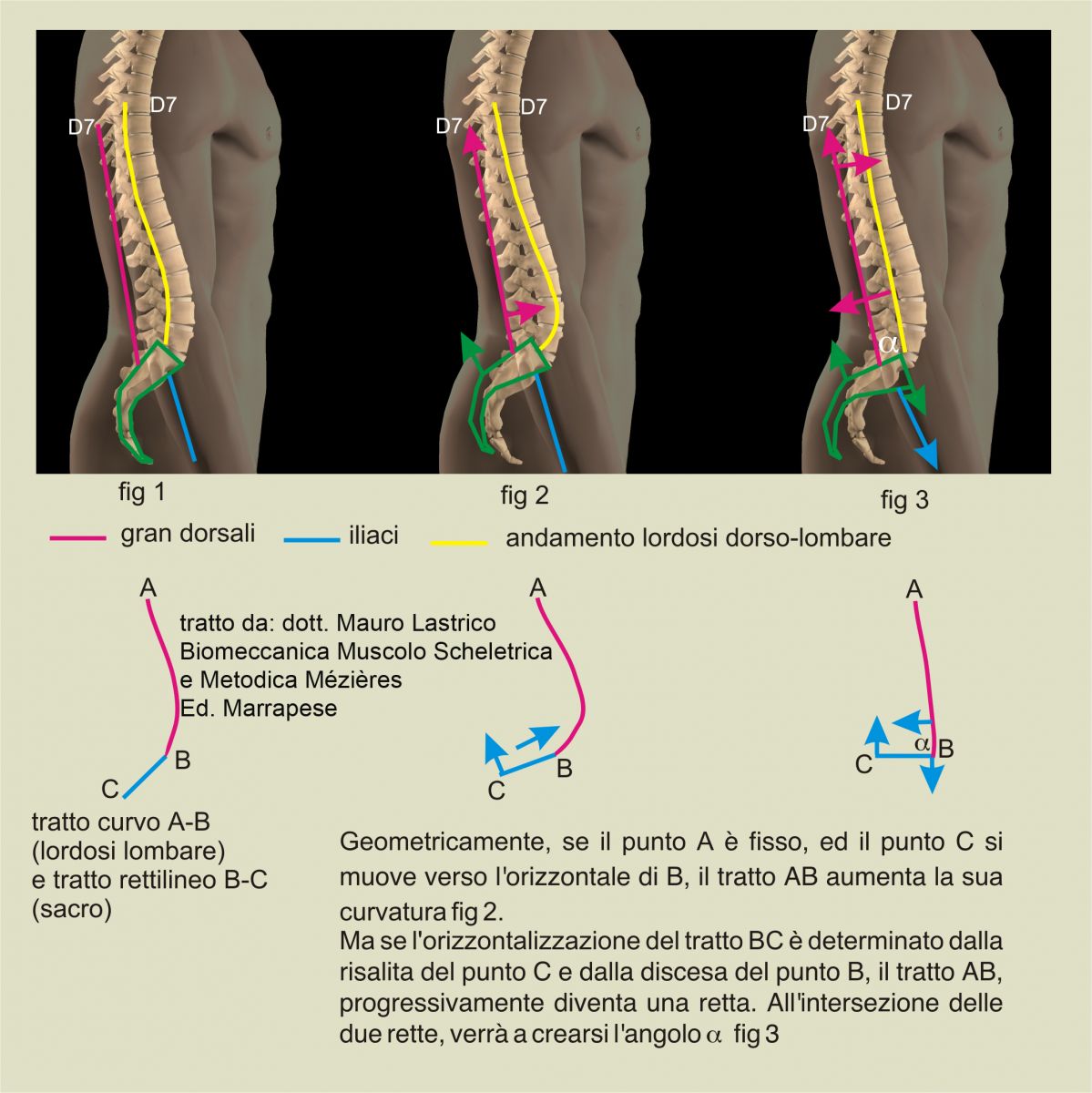
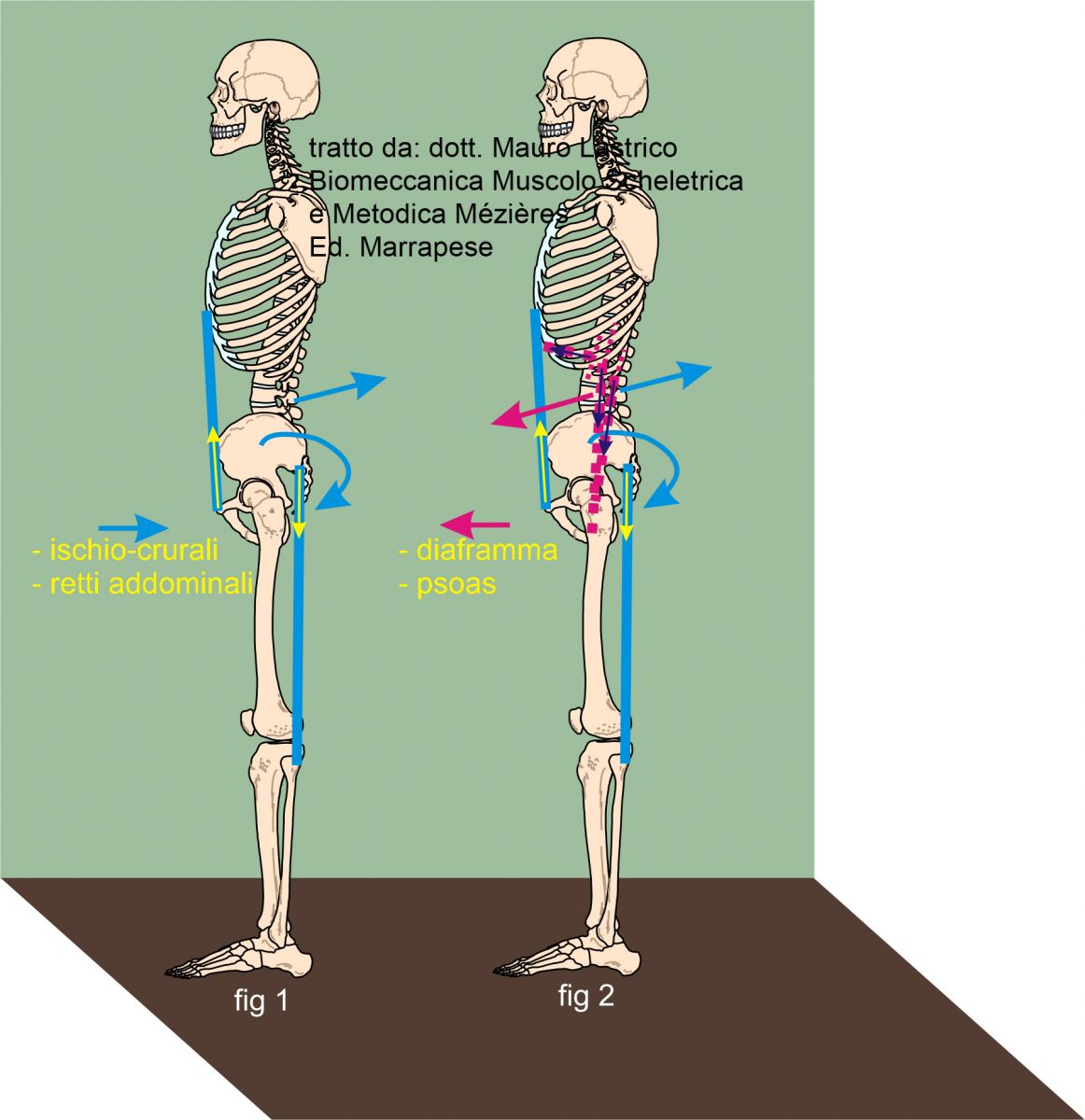
Fig 1 physiological vertebral sinusoid, fig 2 latissimus dorsi and paravertebrals bring the pelvis into anteversion producing initially lumbar lordosis increase. However, if the pelvis is brought horizontal by further traction by latissimus dorsi and iliacs, fig 3, and erect stance is maintained (D7 acts as fixed point), the lumbar-sacral curve is transformed into two straight segments forming an angle at the fifth lumbar vertebra.
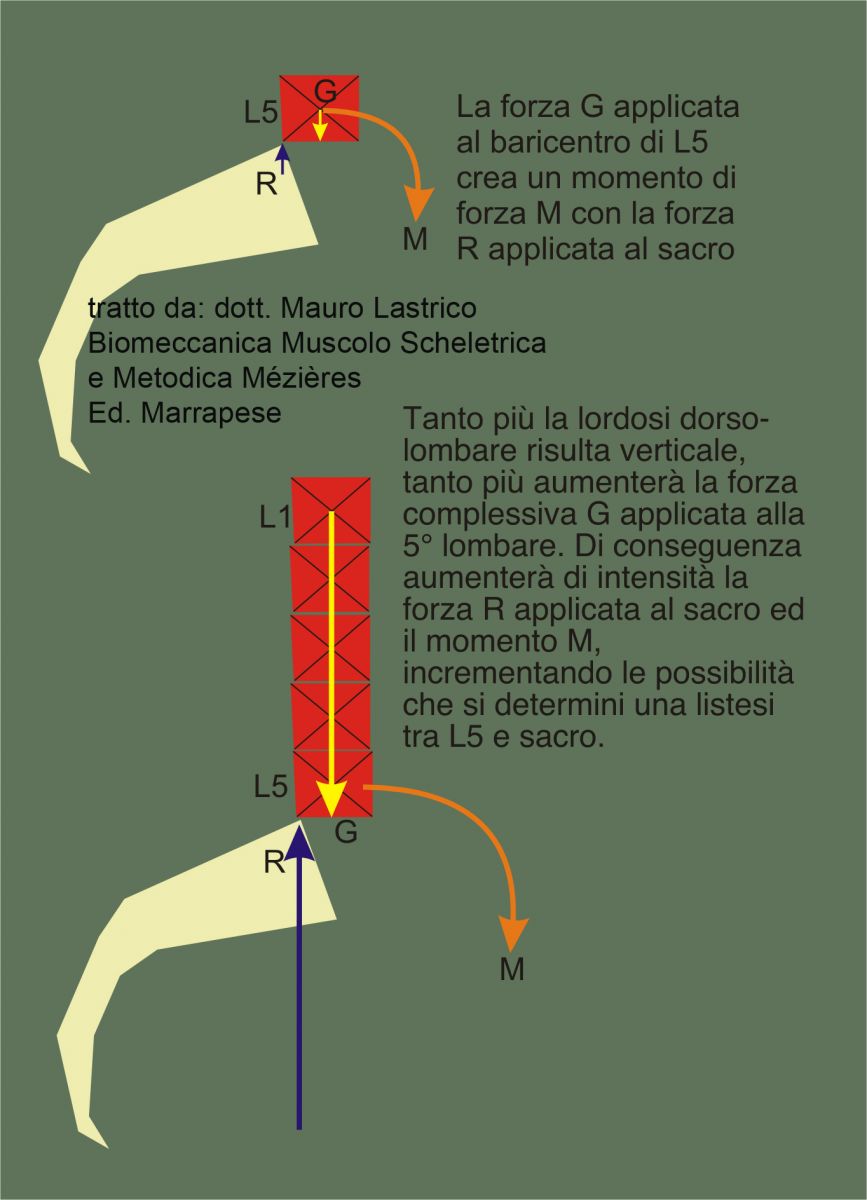
Lumbar lordosis decrease is thus the product of the exacerbation of the traction forces that cause lordosis increase, particularly involving the latissimus dorsi-iliacs pair, which produce a moment of force at the pelvis causing its horizontalization. Moment of force that, as we know, is given by the product of force expressed by latissimus dorsi and iliacs multiplied by their distance between the force application point and the center of rotation.
With sacral horizontalization a moment of force is also generated between sacrum and fifth lumbar caused by forces G and R. This moment, projecting the fifth lumbar anteriorly, may cause spondylolisthesis.
Lumbar spine lordosis may also decrease due to dorsal kyphosis decrease caused by scapular adductors and dorsal paravertebrals,

in this case the lordosis decrease will affect not only the dorso-lumbar tract, but also the cervico-dorsal one.
Pelvis
Its antero-posterior stability is determined by the latissimus dorsi, paravertebrals, iliacs and rectus femoris for anteversion (magenta) and by the hamstrings and rectus abdominis for retroversion (light blue).
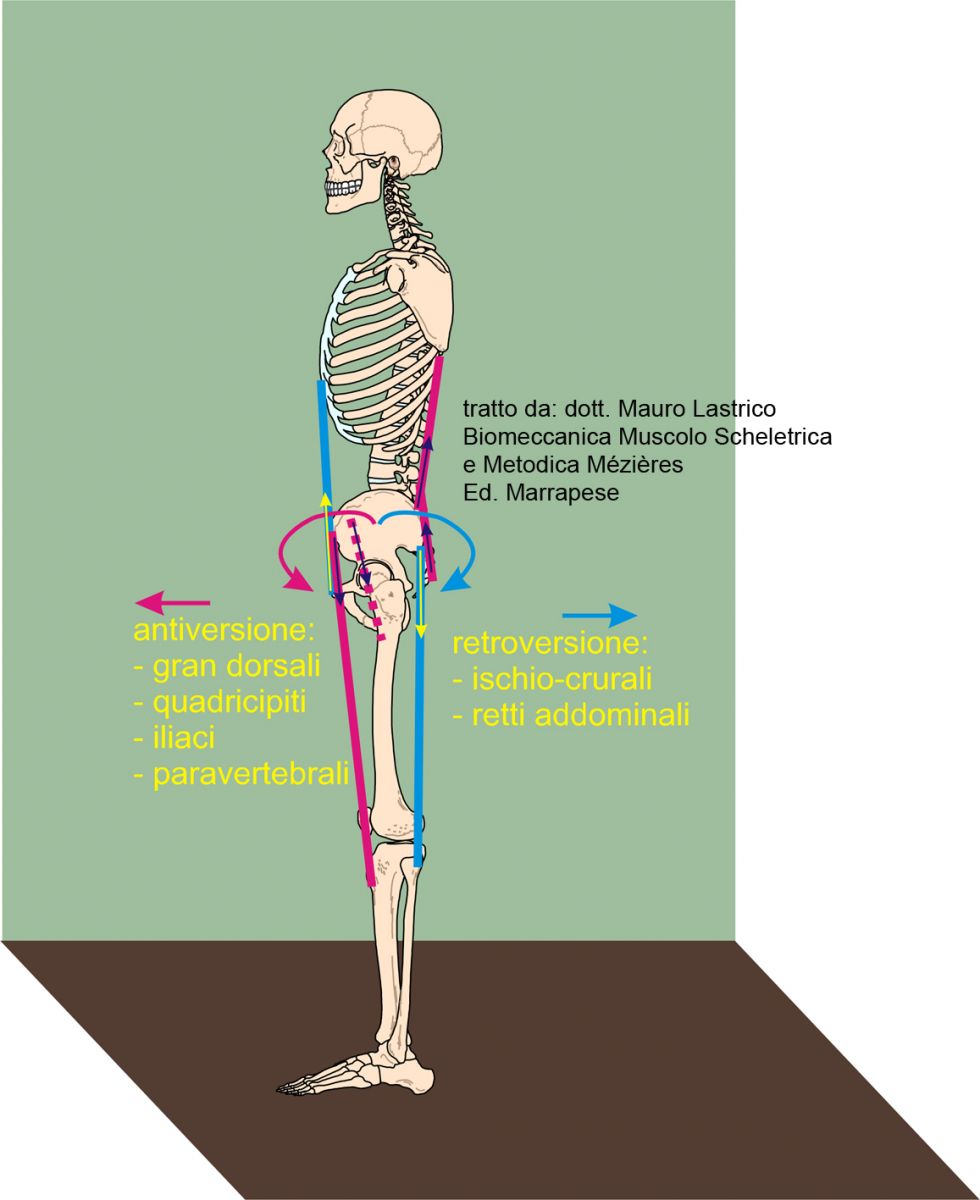
Vectorial force dominance favors anteversion mainly due to the large traction force potentially expressible by the latissimus dorsi.
Clinically, the most frequent patterns are represented either by a broad excess of dorso-lumbar lordosis with pelvic anteversion or by a verticalization of the lumbar tract associated with sacral horizontalization with angular fulcrum on the fifth/fourth lumbar vertebra.
Less frequent are patterns where the dominant vectors are the pelvic retroverters. In this case the pelvis will be retroverted, and the lumbar spine may appear straight due to the mechanical push induced by pelvic retroversion (fig 4.43a) but also hyperlordotic due to the traction effect of the diaphragm/psoas force couple (fig 4.43b). In the latter case, a counteracting force couple acting on the spine is evident, created by the forces of diaphragm and psoas (magenta) and the mechanical force resulting from pelvic retroversion (light blue).
Conclusions
In summary, muscles directly acting sagittally on the cranio-sacral sinusoid in standing can cause:
Skull
- anterior flexion by the action of the sternocleidomastoids
- posterior flexion by the action of the upper trapezius fibers and cranio-vertebral paravertebrals. If the skull is in posterior flexion, the sternocleidomastoids invert their action and become coagonists, since their force line is located behind the mastoid
- anterior projection by the action of the scalenes. Once the skull is anteriorly projected, the anterior neck muscles and sternocleidomastoids assist in its fixation
- posterior projection by the action of the upper trapezius fibers and, if posterior head flexion is associated with increased cervical lordosis, by the action of the levator scapulae and paravertebrals. Since no muscles have extracorporeal insertion, posterior projection of the skull without increased cervical lordosis is possible only through increased dorso-lumbar lordosis or decreased dorsal kyphosis.
Cervico-dorsal lordosis
- straightening through action of the scalenes and anterior neck muscles (rectus capitis anterior, longus capitis, longus colli). The cervical spine is thus projected forward becoming straight and oblique. Alternatively, straightening may be indirectly caused by decrease of dorsal kyphosis: in this case the spine will be straight and vertical.
- hyperlordosis by the direct action of scalenes, levator scapulae and paravertebrals; indirect by posterior head flexion through action of upper trapezius fibers.
Dorsal kyphosis with apex at D5
- straightening through the action of the middle and lower trapezius fibers, rhomboids, dorsal paravertebrals
Dorsal kyphosis with apex between D6 and L1
- accentuation due to the action of latissimus dorsi (insertions on spinous processes from D7 to D12) which project the vertebrae posteriorly and towards the ground.
Dorso-lumbo-sacral lordosis
- straightening as a consequence of sacral horizontalization by latissimus dorsi, iliacs and rectus femoris. D7, for maintaining standing posture, acts as a fixed point. The lumbo-sacral curve is transformed into two straight segments forming an angle at the lumbar fifth vertebra. Lumbar lordosis straightening can also be the mechanical result of pelvic retroversion by combined action of hamstrings and rectus abdominis. Or the skeletal result of dorsal kyphosis decrease with apex at D5
- hyperlordosis by direct action of latissimus dorsi, paravertebrals, psoas, diaphragm, quadratus lumborum.
Pelvis
- anteversion by action of latissimus dorsi, paravertebrals, iliacs, rectus femoris
- retroversion by action of hamstrings and rectus abdominis
Not all patterns have the same likelihood of occurring. Applying vector analysis to acting muscles shows dominances indicating not the only but the most frequent possibilities of action.
Moreover, any modification of a spinal tract, altering the center of gravity, requires involvement and modification of other parts.
In summary, force lines of vectorially dominant muscles acting on skull, vertebral sinusoid, pelvis: