AIFiM M
Italian Association of Physiotherapists for the Study and Development of the Mezieres Method
Advanced Institute of Neuro-Myo-Fascial Biomechanics
AIFiMM Provider ECM n° 1701
The only Mezieres school to have been directly recognized by the Italian Ministry of Health, becoming ECM Provider n° 1701


Biomechanics of the Scapulocostal Relationship
Dr. Mauro Lastrico
Biomechanics: scapulocostal relationship
Dr. Pt Mauro Lastrico
Excerpt from:
"Musculoskeletal biomechanics and Mézières method"
Author: Dr. Mauro Lastrico
Marrapese Publisher
The acting muscles can determine a "shoulder" positioned high, low, anteriorly, or posteriorly.
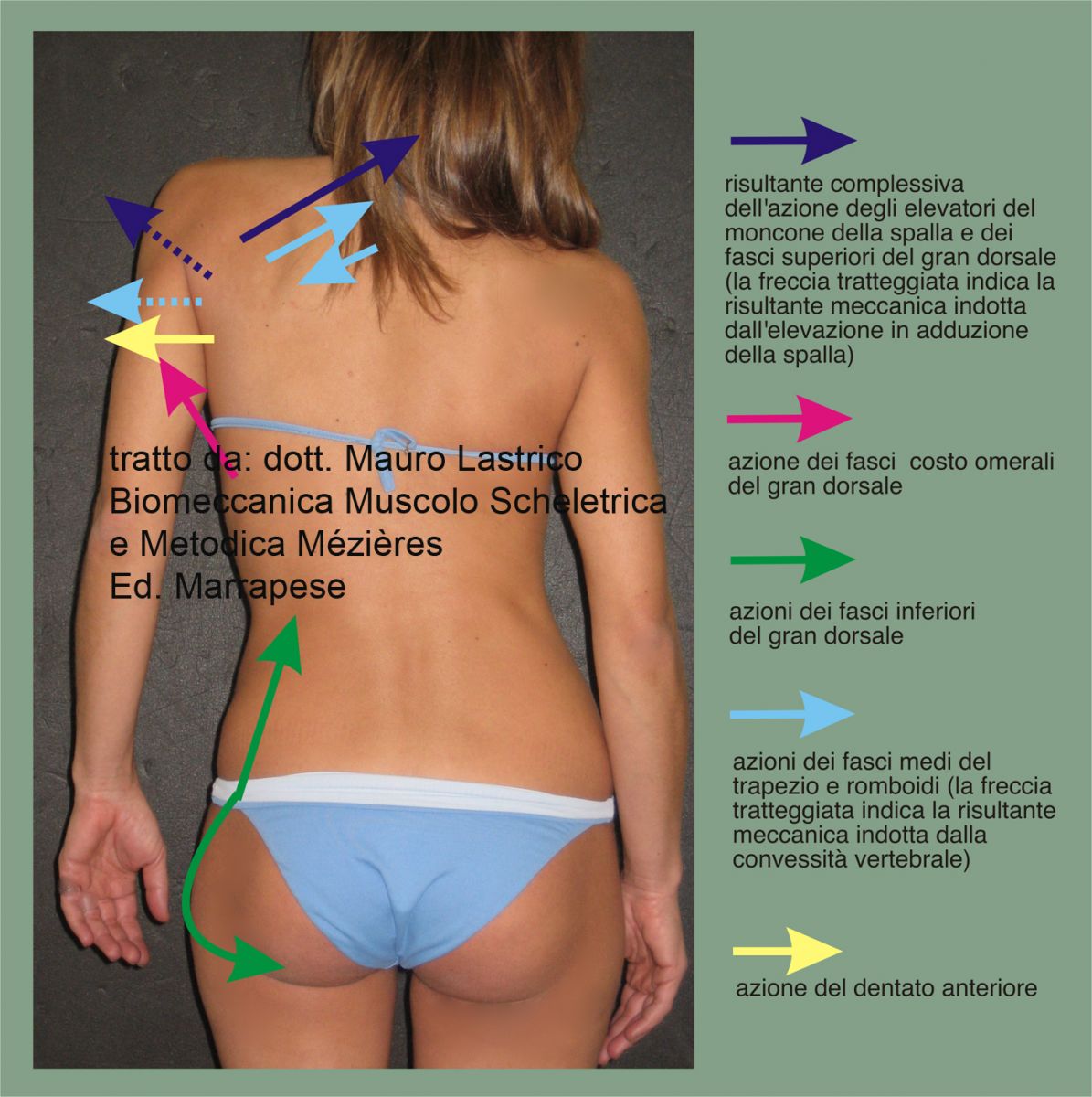
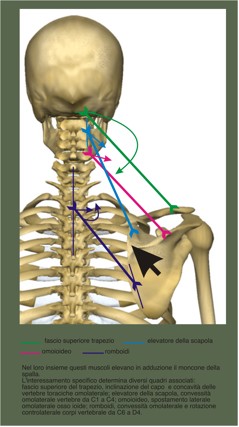
High shoulder
Mainly determined by the sum of the latissimus dorsi and the cranio-cervico-thoraco-scapular muscles or only the latter.
Modest elevation caused by the middle fibers of the trapezius.
The clavicle will have an ascending trend.
If the latissimus dorsi is involved, there will be an associated greater lateral thoracic convexity and elevation of the ipsilateral hemipelvis.
Among the cranio-cervico-thoraco-scapular muscles, different associated patterns will appear depending on the dominant muscle:

Since all acting muscles work in summation, associated patterns can occur.
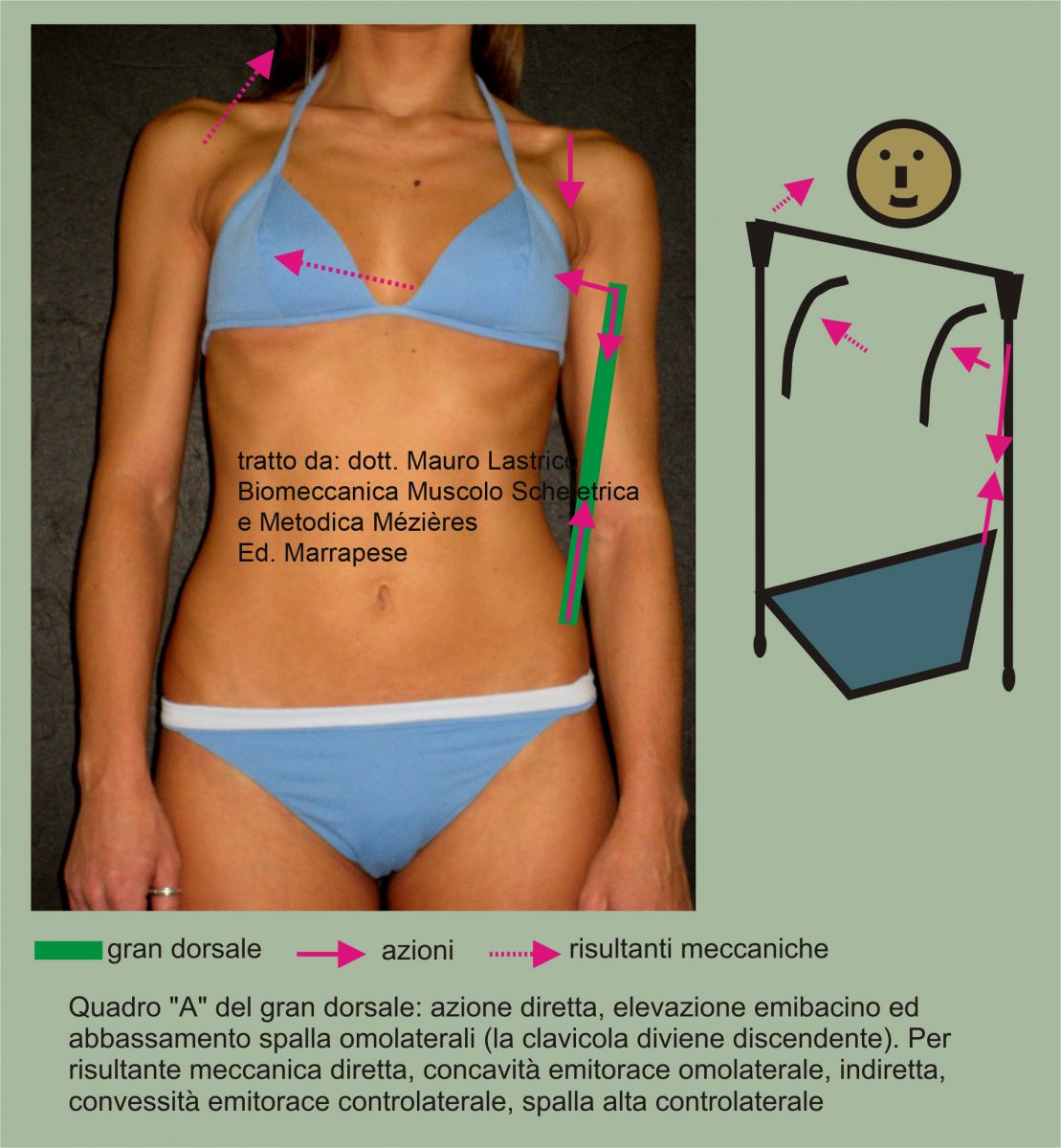
Low shoulder
Determined by the ipsilateral latissimus dorsi, associated with ipsilateral lateral thoracic concavity and ipsilateral elevated hemipelvis.
The clavicle will have a descending trend.
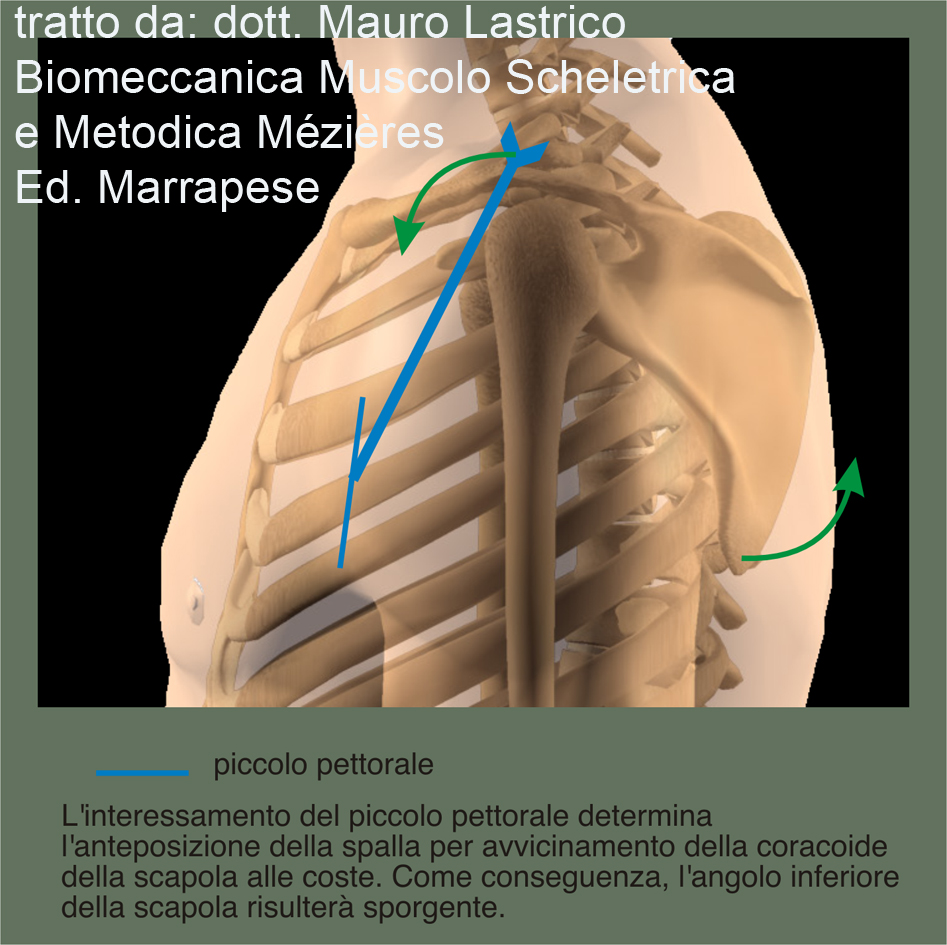
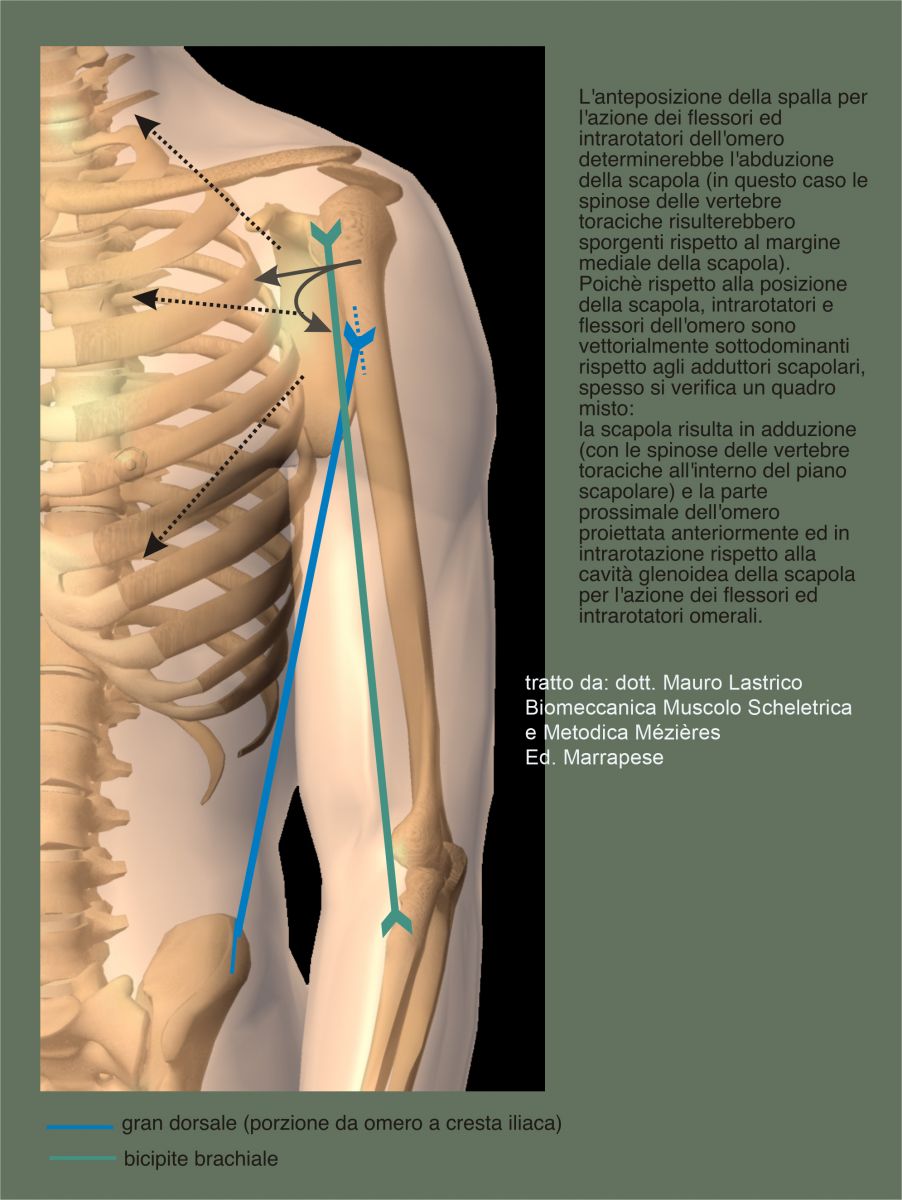
Anterior shoulder
Dominant vectors are represented by: the humeral internal rotators with the humerus internally rotated; the biceps brachii and coracobrachialis, with the elbow flexed; the pectoralis minor, with increased anterior convexity of the ribs from the third to the fifth and the posterior prominence of the scapula's inferior angle.
Since the internal rotators and humeral flexors are vectorially subordinate to the scapular adductors, clinically the apparent anterior shoulder often presents a dissociated pattern: the humeral head is anterior and internally rotated, scapula adducted.
Posterior shoulder
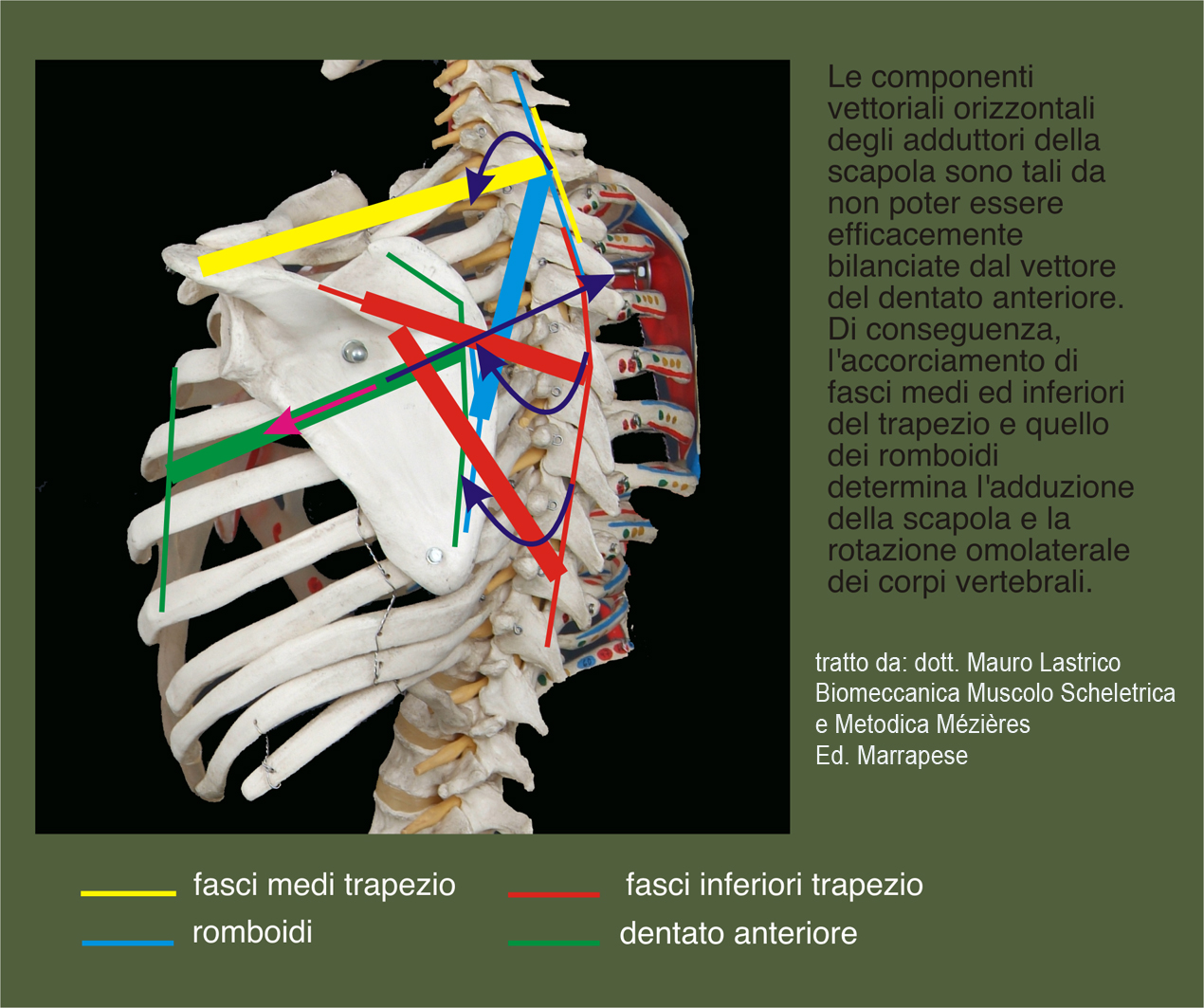
Determined by the scapular adductors (rhomboids, middle and lower trapezius fibers). The scapula will be adducted and posteriorly prominent relative to the spinous processes of the thoracic vertebrae. The thoracic vertebrae may show ipsilateral convexity due to contralateral rotation of the vertebral bodies.
The antagonist muscle to adduction, the serratus anterior, is vectorially subordinate.
The scapula is "resting" on the rib cage and under physiological conditions should be positioned at the side of the thorax with the medial border aligned with the spinous process of D5.
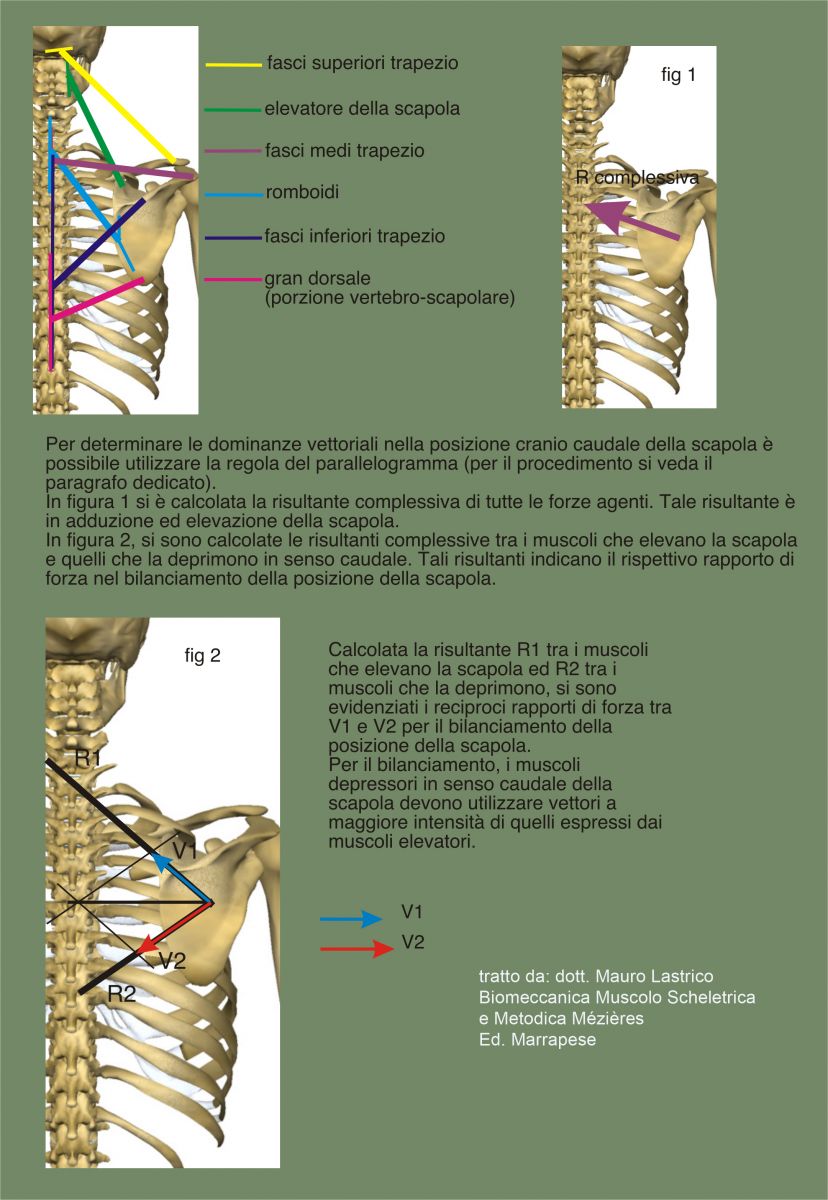
In the cranio-caudal direction, the scapula position is maintained by the antagonistic action between the muscles that elevate and depress it.
In the latero-lateral direction, the scapula position on the thorax is maintained by the action of the scapular adductors (rhomboids, middle and lower trapezius fibers, portion of latissimus dorsi connecting thoracic vertebrae to inferior scapular angle and humerus) and the serratus anterior which abducts it (extending from the first nine ribs to the entire medial border, to the superomedial angle and inferior angle of the scapula).
The force lines of the serratus anterior are shorter and smaller than those expressed by the scapular adductors, thus the serratus anterior is subordinate.
The dominant action on the scapula is vertebral adduction.
The medial border of the scapula is prominent and posterior to the spinous process of D5, not due to weakness of the serratus anterior but due to the excessive tension of the adductors projecting anteriorly the thoracic vertebrae from D3 to D6 and consequently the ribs.
It is not the scapula that "protrudes" but the vertebrae and ribs that "enter".
The prominence of the medial border of the scapula is also determined by the increased tension of the serratus anterior caused by its attempt to oppose the traction force exerted by the adductors.
In patterns where the shoulder is anteriorly positioned, it is necessary to differentiate between the position of the humerus and that of the scapula: often the shoulder appears anterior due to humeral internal rotation, while the scapula is adducted.
Copyright © 2025 AIFiMM Formazione Mézières Provider E.C.M. n. 1701. All rights reserved.