AIFiM M
Italian Association of Physiotherapists for the Study and Development of the Mezieres Method
Advanced Institute of Neuro-Myo-Fascial Biomechanics
AIFiMM Provider ECM n° 1701
The only Mezieres school to have been directly recognized by the Italian Ministry of Health, becoming ECM Provider n° 1701


Biomechanics of the Knee
Dr. Mauro Lastrico
Biomechanics: knee
Dr. Pt. Mauro Lastrico
Excerpt from:
"Musculoskeletal biomechanics and Mézières method"
Author: Dr. Mauro Lastrico
Marrapese Publisher
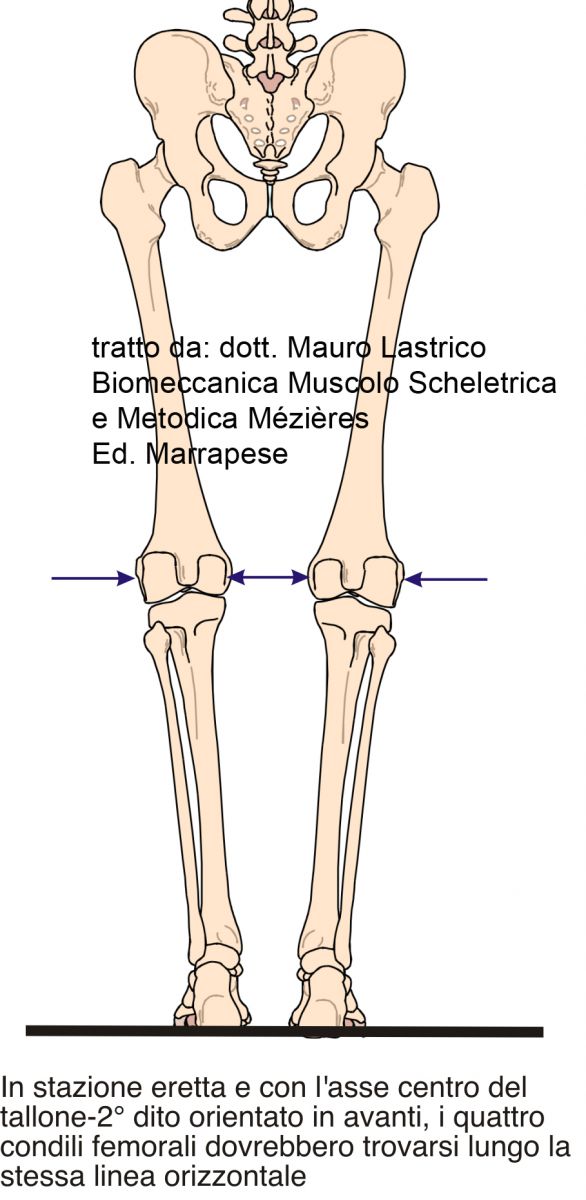
In standing position and posterior view, with the center axis from heel to second toe oriented forward, the four femoral condyles should align on the same horizontal line.
Axial deviations of the knee joint on a muscular basis can produce various clinical pictures, differently associated:
Hyperextension
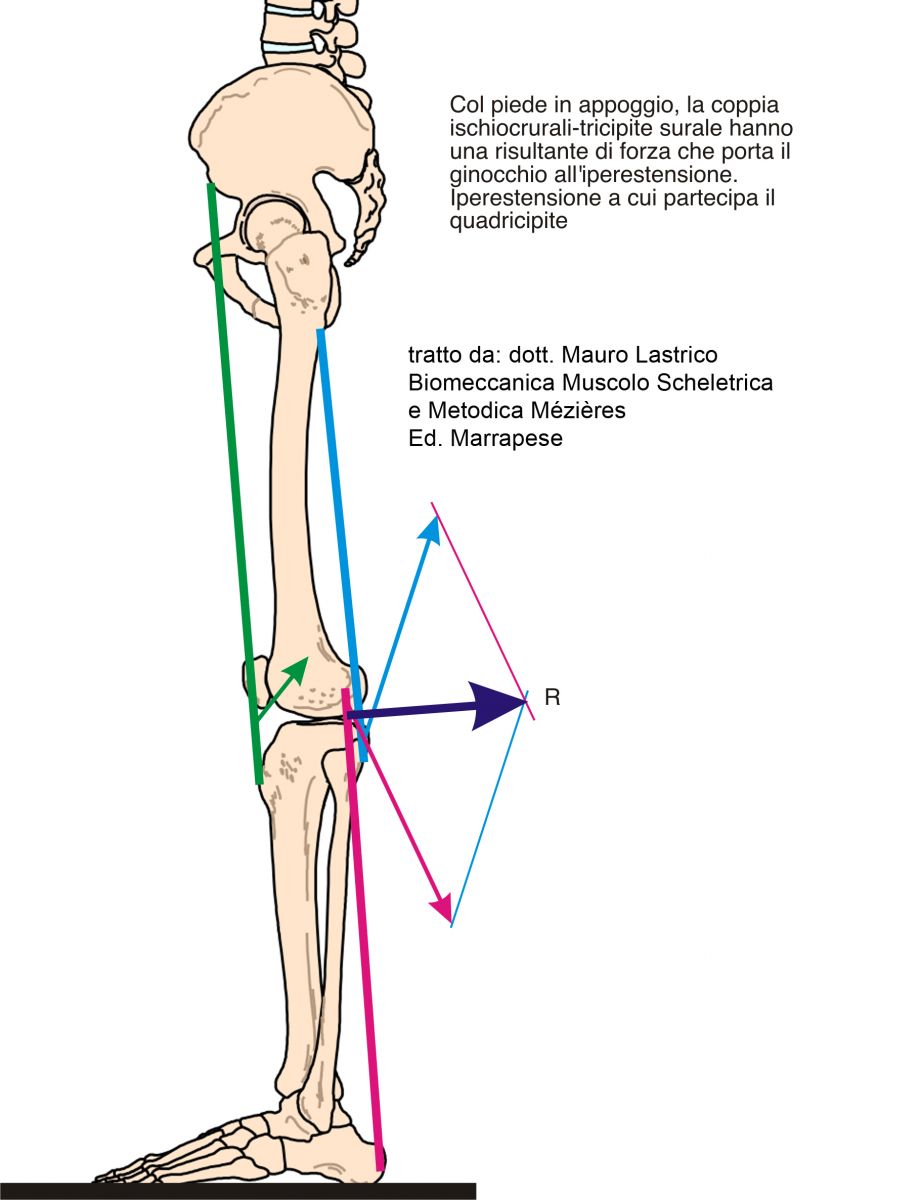
In standing position with the foot fixed on the ground, the hamstrings and triceps surae change their action from knee flexors to extensors.
The quadriceps and adductor magnus participate in this action.
When the foot is fixed, such as rising from a seated position or during the stance phase of gait, the four muscle groups act as coagonists for knee extension. However, due to a favorably oriented line of force, the action is mainly performed by the hamstrings-triceps surae pair.
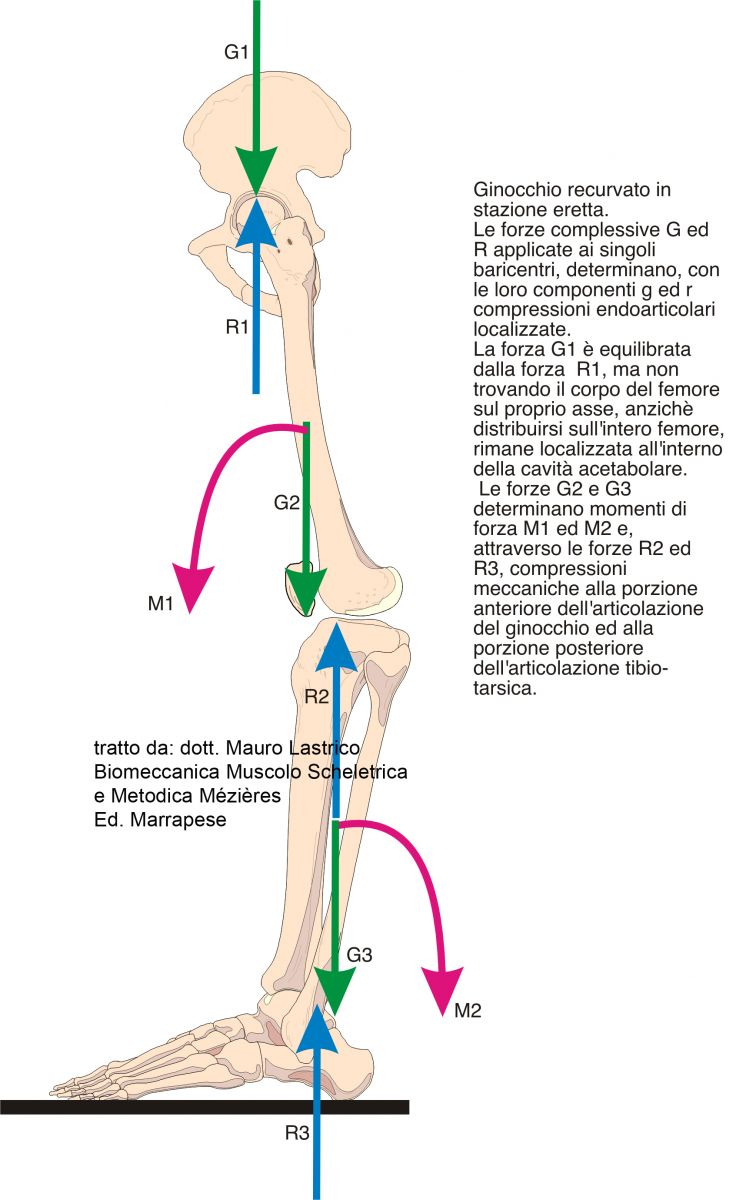
The joint misalignment of the knee also causes alterations in the hip and ankle joints, detectable through the study of forces G and R.
In particular, the total force from the trunk applied to the hip joint cannot be distributed over the entire femur, as it is extended. Consequently, forces G and R will concentrate within the acetabular cavity causing potential mechanical conflicts.
A-physiological moments of force may also develop at the knee and ankle joints.
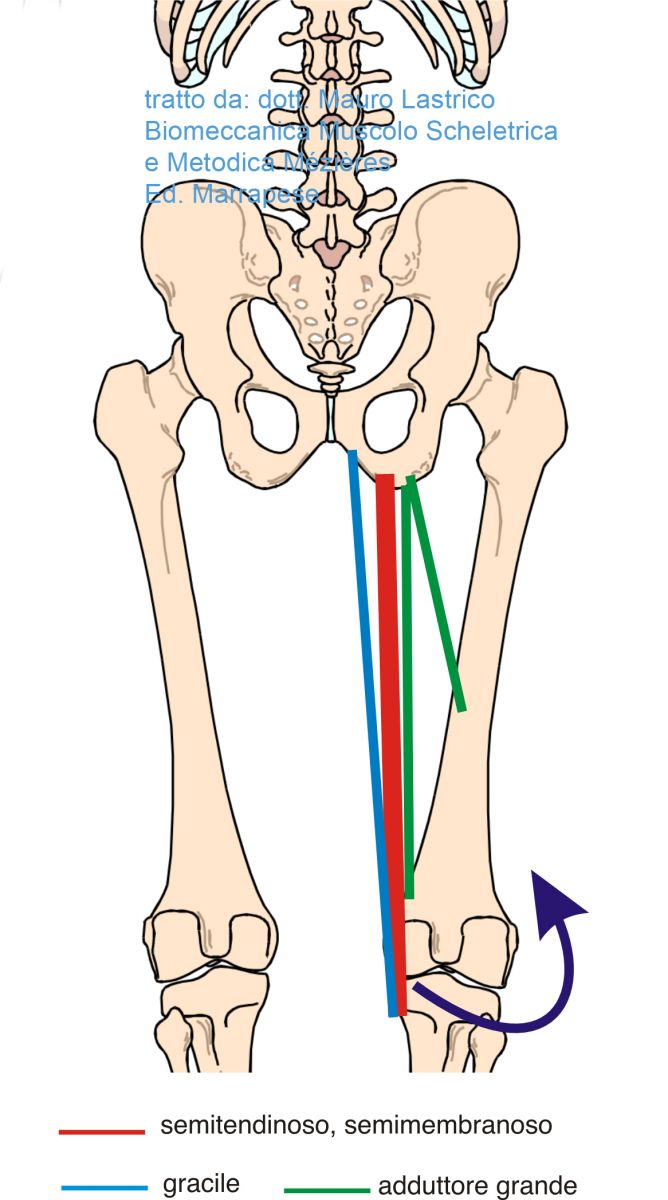
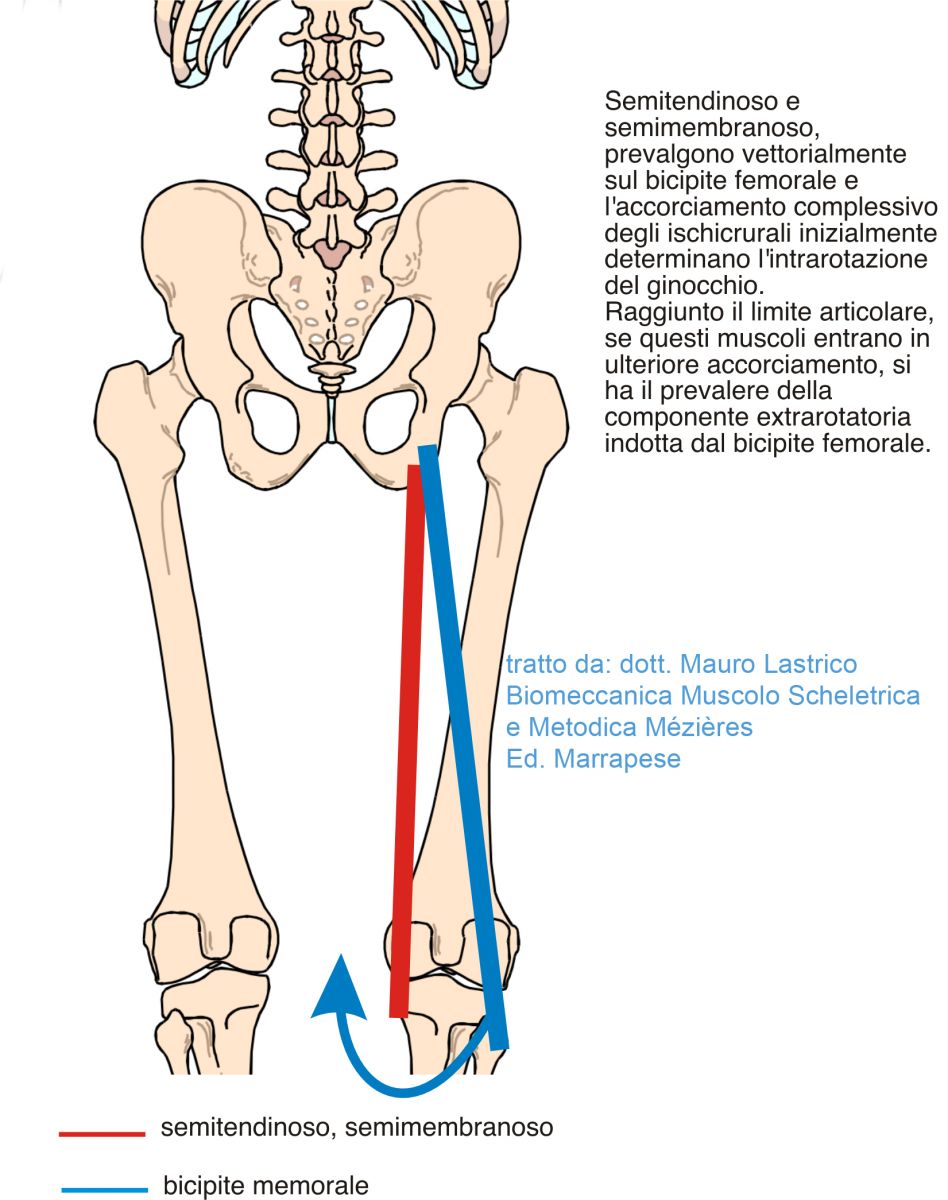
Internal rotation
Under load, the dominant vectors are those of semitendinosus and semimembranosus, associated with femoral adductors having an internal rotation component.
Hyperextension and internal rotation often compose an associated picture.
To differentiate recurvatum caused by muscle shortening from ligament laxity, among many investigations, it is possible to actively or passively derotate the knees. In the case of recurvatum due to ligament laxity, derotation does not modify hyperextension; if caused by muscle shortening, derotation results in knee flexion.


Flexion
The hyperextensive action of the hamstrings-calf pair is limited by the femorotibial joint. Once this limit is reached, if the shortening of the two muscle groups progresses, the final resultant line of force causes knee flexion.
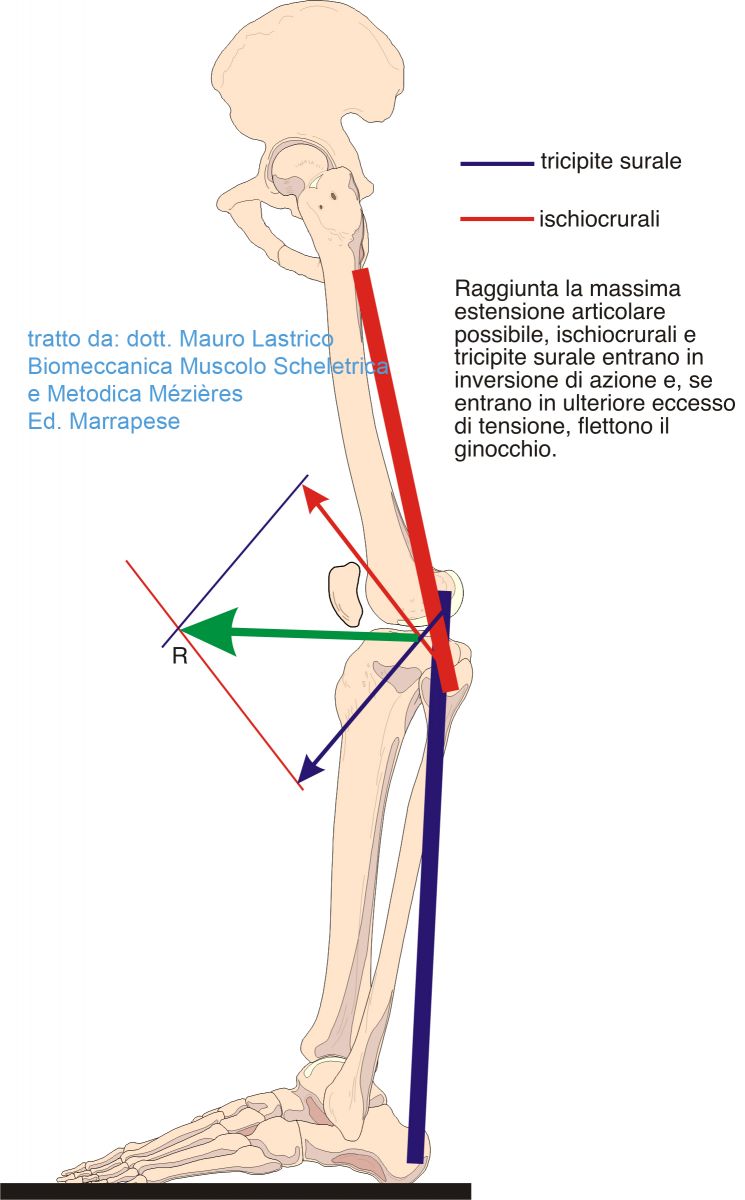
If the shortening of the hamstrings-triceps surae pair is such as to bring the knee from hyperextension to flexion, the two muscle groups return to being knee extensors. In this case, however, their vertical vector components act with an intensity such as to prevent extension itself.
The sum of the vertical vector components will not allow the knee to extend while standing but, in cooperation with the quadriceps, will oppose falling to the ground. This action requires great energy expenditure with consequent joint stiffness.
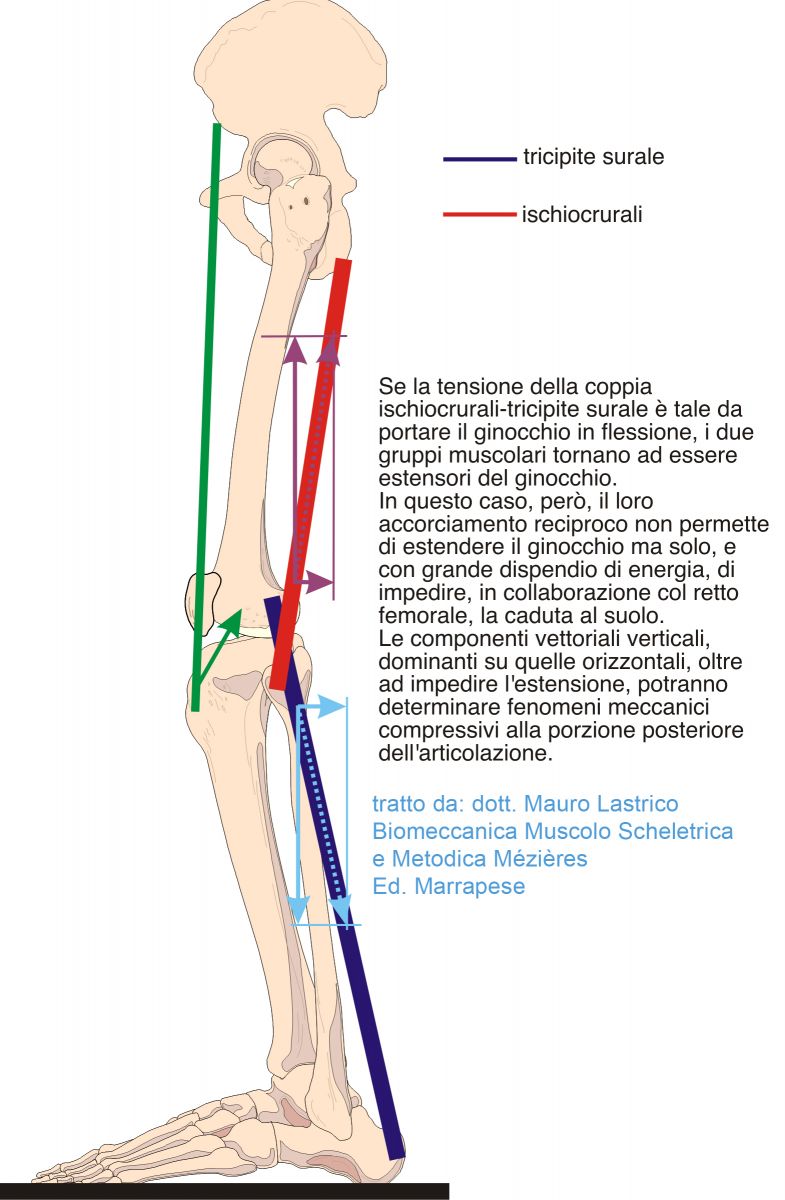
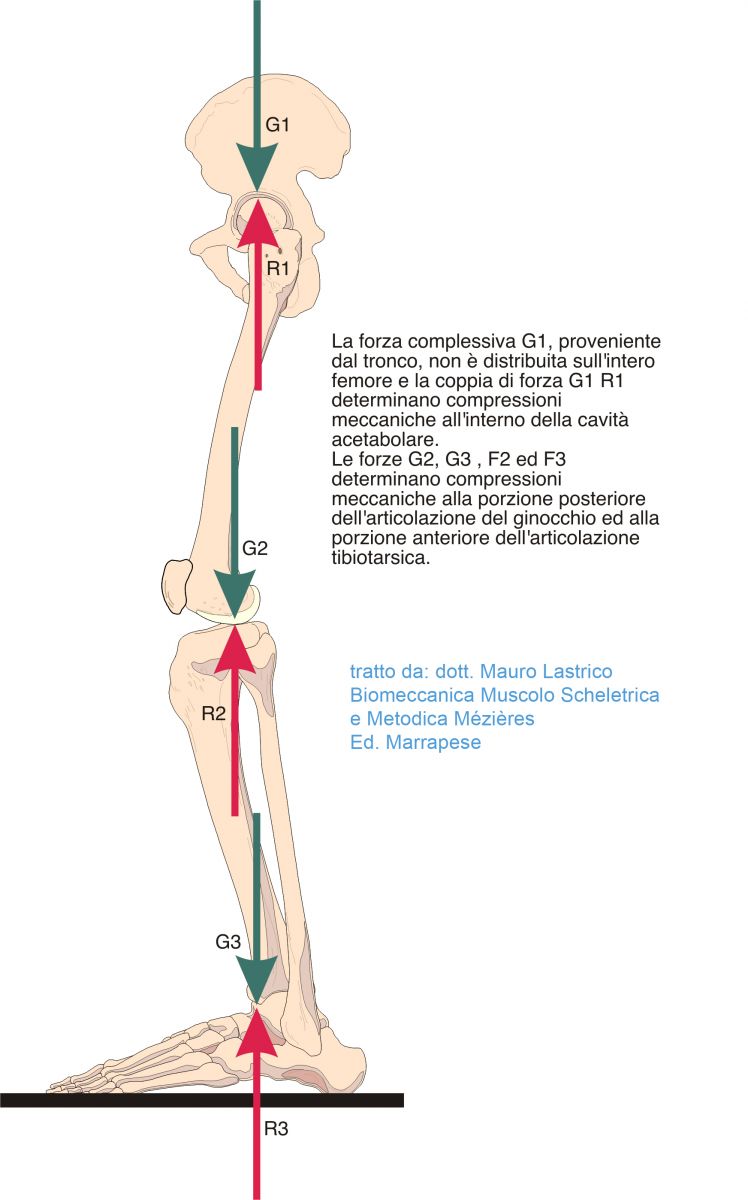
The total forces G2, G3 and R2, R3 and their components g and r may cause compressive phenomena localized to the posterior portion of the knee joint and the anterior portion of the ankle joint.
The total force G1, coming from the trunk, not being able to distribute evenly over the entire femur, will be balanced by the total force R1 inside the acetabular cavity, giving rise to potential intra-articular mechanical conflicts.
External rotation
Internal rotation is limited by the joint itself. Once this limit is reached, the hamstrings further shorten, and the external rotation component of the biceps femoris prevails, associated with the external rotators.
The four patterns of knee axis alteration described above are associated and represent a progression of worsening: initially internal rotation and hyperextension, then flexion and external rotation. A knee that appears well positioned may really be so, but it may also have exhausted the first two directions of movement, evolving into the last two.
The two patterns have as extremes internal rotation and recurvatum on one side and external rotation and flexion on the other.
In the transition from one extreme to the other, the muscle components may cause intermediate patterns, variably associated (e.g., the knee may be internally rotated and flexed).
Moreover, since the progression expresses further muscle shortening, the knee joint will become progressively stiffer and intra-articular compressive components will increase.
Lateral patellar deviation
During gait, the patellae must be oriented forward, ensured by the quadriceps femoris.
If due to the action of the hamstrings the femur is internally or externally rotated, the quadriceps can reposition the patella creating femoro-patellar dissociation. The quadriceps action is secondary and aimed at preserving its function.
Patellar deviation is thus directly caused by the quadriceps femoris but as a consequence of the lower limb rotation predominantly induced by the hamstrings.
In the observation of knees, the posterior view provides the effective axial position of the femoro-tibial relationship and the femur, while the anterior view allows assessment of patellar position and its synchrony with femoral rotation.

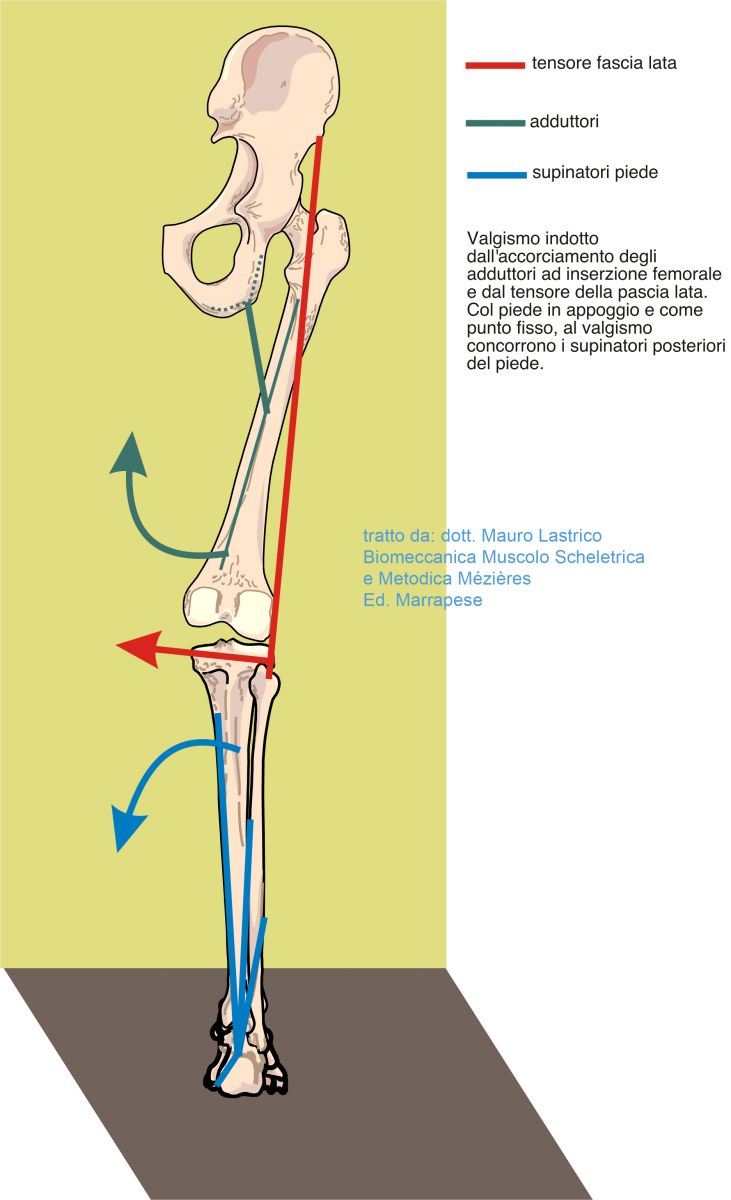
Valgus
The muscle force couple that can cause valgus when shortened consists of the femoral adductors (which deviate the femur inward) and the tensor fascia latae (which displaces the distal tibia outward).
Under load (foot as fixed point), the foot supinators originating from the posterior tibia contribute.
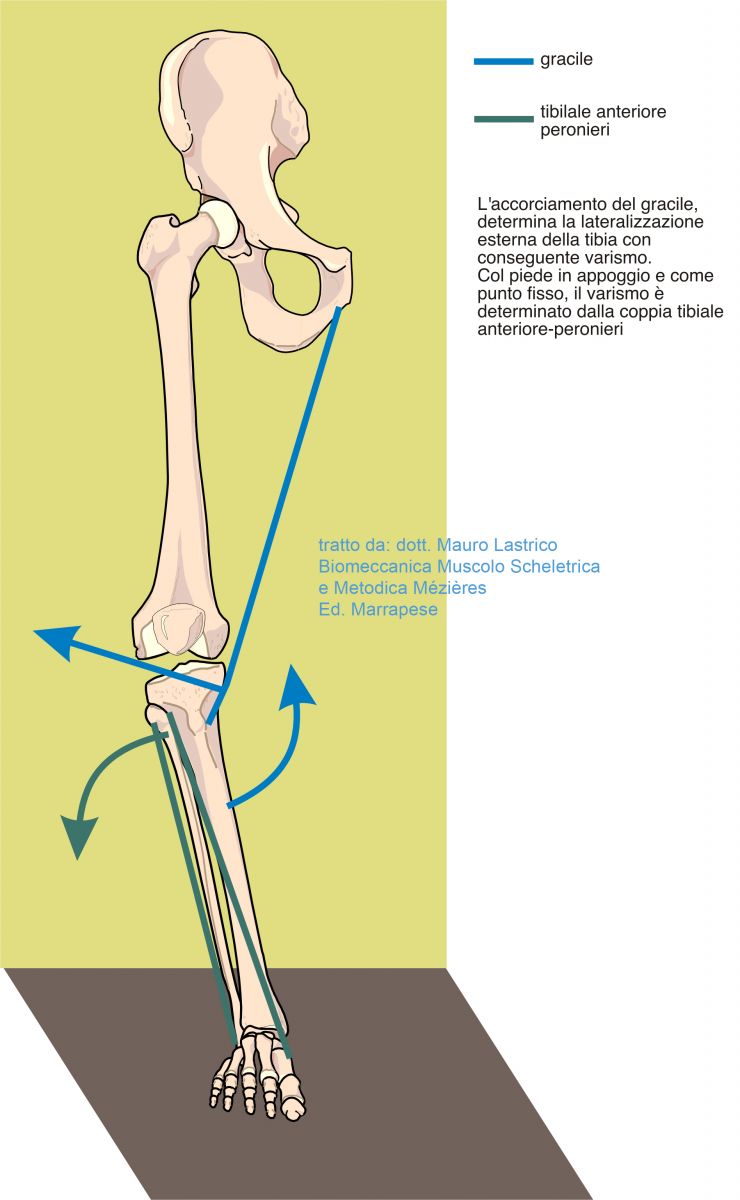
Starting at the femur, the muscle vector that can cause varus when shortened is given by the gracilis muscle (which deviates the tibia outward).
Under load (foot as fixed point), foot supinators originating from the anterior and lateral tibia contribute.
In standing position, with feet together, the medial femoral condyles should slightly touch.
In valgus the contact will be excessive, while in varus contact will be absent.
If varus and valgus are misalignments expressed on the frontal plane, the rotational components of the femur can disguise, by excess or decrease, the real varus/valgus.
To observe the real components of varus or valgus, the lower limbs must be actively or passively derotated in extension.

Copyright © 2025 AIFiMM Formazione Mézières Provider E.C.M. n. 1701. All rights reserved.