Biomechanics: Characteristics of Complex Systems
Dr. Mauro Lastrico
Biomechanics: characteristics of complex systems
Dr. ft. Mauro Lastrico
Extract from:
"Musculoskeletal Biomechanics and Mézières Methodology"
Author: Dr. Mauro Lastrico
Marrapese Publisher
* in a complex system all the elements that compose it are interdependent and interacting
This means that any segmental corrective action, localized to a body district, will cause adaptations in adjacent districts.
These adaptations could be corrective or negligible in extent, but they could also be aggravating, with the aggravation greater than the correction applied.

During the examination it is therefore necessary to generally observe the effect of the corrective action, whether it is active, passive or induced by an external means (braces, corsets, insoles, bite, etc).
* understanding the functioning of a complex system can only happen by considering the system as a whole;
this means that to correctly interpret the meaning of the segmental strategies, both static and dynamic, that the system implements, it is necessary to observe the connections between the altered district pattern and the overall patterns.
It also means that the symptom can be an expression of local suffering, referred pain, or postural discomfort. Differentiation can occur through comprehensive musculoskeletal analysis and by using analytical and systemic tests to detect interfering dominances on posture, distinguishing between primary and secondary muscle shortenings.
* a complex system, in pursuing its objectives, is capable of generating solutions not predictable from the examination of individual elements, that is, it can generate "emergent abilities";
this third characteristic has very important therapeutic implications. It basically says that when performing an action, the muscles anatomically assigned may not necessarily be used, but can be replaced by others that according to linear mathematics vector analysis should/could not come into play. These are called substitution moments.
These moments manifest in two occasions:
1. physics tells us that force couples compared to single forces have the advantage of performing better work and overall use less energy.
Almost all muscles, when performing an action, can rely on synergists (force couples), while others are "isolated" and vectorially subdominant in their action as agonists or antagonists. Among these: rectus abdominis, for the anteroposterior descent of the chest in the active expiratory act; pectoralis major, in shoulder anteposition; rectus femoris, in anteropulsion of the ipsilateral hemipelvis during walking; suprahyoid muscles, in mouth opening; etc.
The cortical centers (pyramidal system) identify the movement objective, i.e. the "what", while the "how" is under the control of subcortical centers (extrapyramidal system), through a mapping called "body schema".
The "what" has priority over the "how".
If the antagonists to the target movement are in excess resistant force, i.e. shortened, the isolated muscles are in vectorial subdominance and unable to perform the action. Since the action prevails over the execution mode, these muscles will be replaced by others that will allow a targeted action but in alteration of the physiological skeletal movement.
Examples: if inspiratory muscles are increasing in resistant force and shortened, the rectus abdominis is unable to cause thoracic descent for active expiration. This action will therefore be performed by the sum of interventions of the latissimus dorsi, transverse abdominis and oblique abdominis. The "what" will be expiration, but the "how" will occur with the closure towards the median line of the hemithoraxes and, due to the involvement of the latissimus dorsi, increase of dorso-lumbar lordosis.
In the retraction of the mandibular serratus (temporalis, masseter and internal pterygoid), the function of the suprahyoid muscles in mouth opening is performed by the external pterygoids, whose physiological action is to control lateral movements of the mandible. The "what" will be mouth opening, but in the "how" the mandibular condyles will no longer descend along the temporal fossa eminence, but will be "torn" forward causing subluxations or dislocations of the temporomandibular joint.
A similar investigation methodology will be applied to the other "isolated" vectors.
Substitution strategies prove useful and indispensable in the "here and now" to allow the function at the best of possibilities, but their use causes mechanical conflicts over time with the onset of symptoms distant from the place of origin. For example, low back pain can be caused by a thoracic block, in turn caused by the retraction of inspiratory muscles forcing the latissimus dorsi to substitute the rectus abdominis, causing a mechanical conflict at the lumbar vertebrae.
Therapeutically it is therefore important to detect the substitution strategies in place and create conditions so that the isolated muscles resume their anatomical function. This is achievable through the re-lengthening of the "brake" muscles, i.e. those in excess resistant force, so that subdominant muscles become free and automatically reinserted into systemic functioning.
2. In the treatment of the a priori and a posteriori antalgic reflex, defensive strategies of the subcortical centers have been highlighted, which use muscle contraction and muscle block on structurally free joints to prevent latent conflicts from manifesting.
Absence of pain is therefore not necessarily synonymous with absence of pathology. Nor is it said that a therapy that removes a symptom will not subsequently cause the appearance of a more severe conflict.
The second line of investigation on substitution moments is aimed precisely at identifying non-mechanical but muscular joint blocks, aimed at non-latent manifestation of direct or indirect mechanical conflicts. This means identifying subjective "protective" strategies.
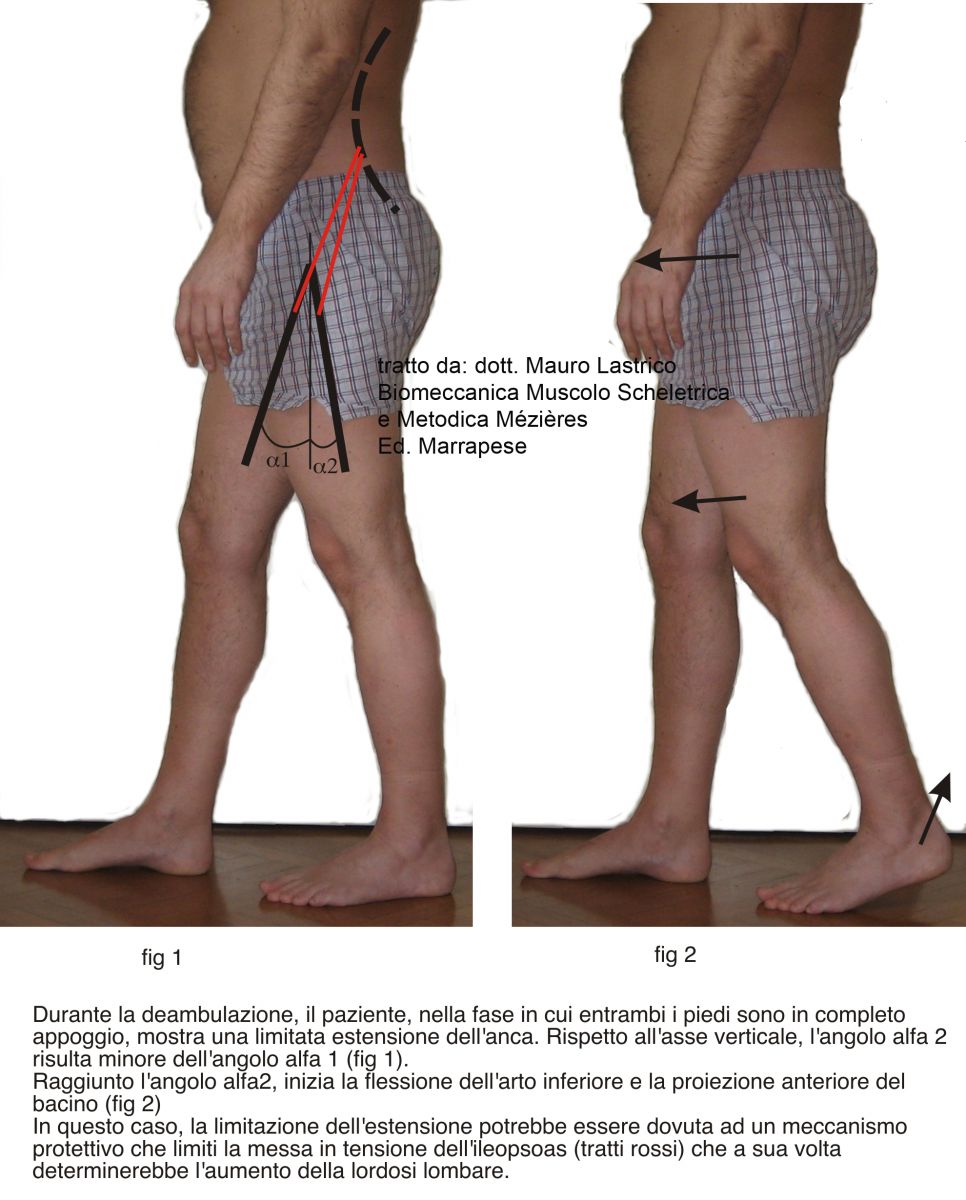
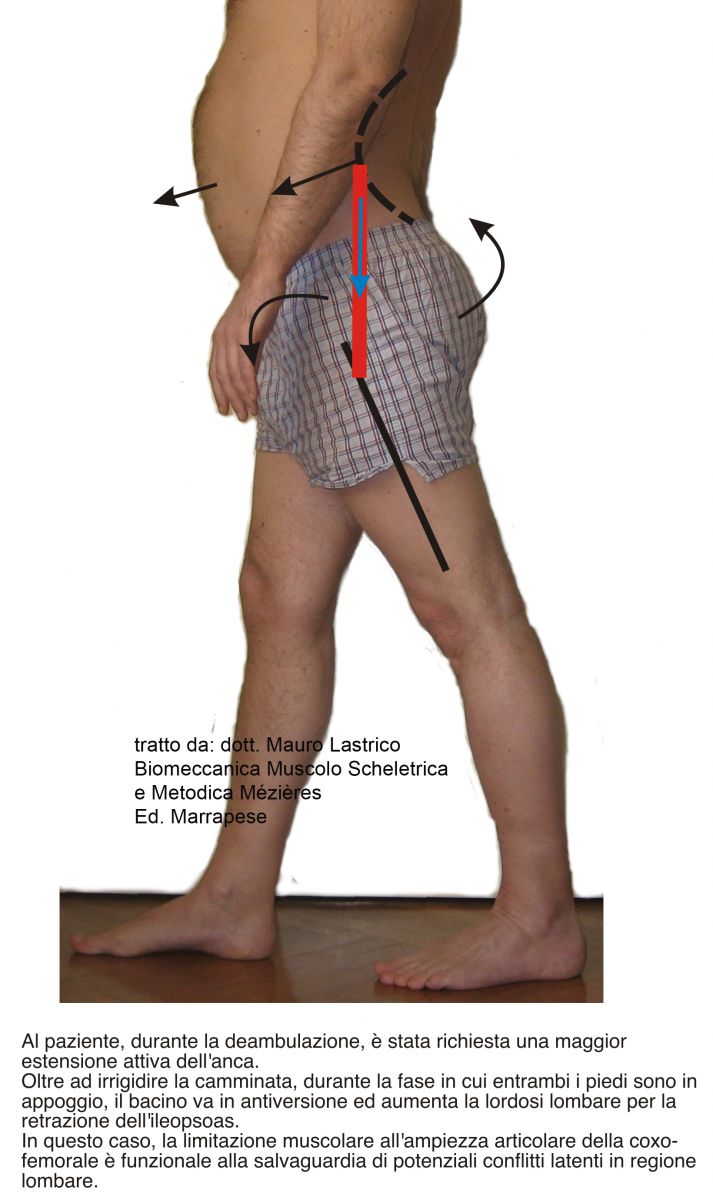
In the analysis of walking, for example, there could be a decrease or absence of posterior femur projection in the support phase in the absence of a coxo-femoral joint problem. This could be determined by a protective strategy that prevents the (retracted) iliopsoas from pulling the spine anteriorly, revealing a latent conflict at the lumbar vertebrae. In this case, the muscular protective strategy uses movement limitation at one joint to safeguard another. However, if the mechanism persists over time, the muscular block can transform into an articular block, causing the appearance of a new pathological picture.
* a complex system makes the best use of its energy when it stands at the "edge of chaos", meaning the elements of stability and dynamism are in such balance as to allow small signals to modify the state of the system.
One of the prerogatives of complex systems is adaptability and the "edge of chaos" is the place where there is enough innovation to give life to a dynamic system and enough stability to prevent it from collapsing into anarchy. If a living system approaches the edge too closely it risks falling into incoherence, but if it retracts too much it becomes rigid.
The physiological vertebral sinusoid and the physiological systemic articular succession are possible only if there are no specific structural alterations and if all muscles work under ideal length conditions. In these conditions, the musculoskeletal system is "at the edge of chaos" because, through small signals, it can guide different behaviors while saving energy. It can, for example, switch from static to dynamic phase with a small shift of a body segment. If the system is "rigid", the energy required to determine the G and R couple favoring dynamics will have to be higher.
If the muscular system is increasing in resistant force due to excess basal tone of the contractile component and if this condition persists over time, the connective portion of the fiber is involved, with shortening of the muscle length itself (primary muscle shortening). A similar mechanism can occur as a consequence of dysfunction of another system (secondary muscle shortening).
In both cases, the consequence will be misalignment of individual skeletal barycenters and loss of muscle dynamic capacity. The system enters a feedback loop: the misalignment of individual skeletal barycenters requires greater basal contraction for maintaining standing posture and for dynamics, the increase in basal tone causes muscle shortening with consequent further misalignment of the barycenters and modifications of the sinusoidal course of the spine and axiality of all other joints.
The system moves away from the "edge of chaos" and becomes rigid.
Walking
In the analysis of walking, all the "pathophysiological" and "abnormal physiological" components will be detected, trying to identify whether these reactions are determined by protective or substitution mechanisms.
To this end, specific and nonspecific parameters will be considered.
Nonspecific parameters
Include: speed, intensity and occupied space.
The importance of these parameters, inherently subjective, is related to whether or not their manifestation is coerced.
Many people, when they find themselves modifying their natural speed (slowing down to look at shop windows, for example) complain of the appearance of musculoskeletal discomfort. In these cases the adopted speed is not free but functional and coerced by the need not to trigger latent problems.
Everyone has their own "natural" rhythm and, if the system is in good skeletal and muscular balance, it can vary it responding to the needs of the moment, without triggering conflicts.
* By speed: the walking speed is meant and it is assessed whether this is excessive or reduced, free or coerced.
* By intensity: it is meant whether the mode with which the walk is expressed is more or less rigid.
* By spatiality: during walking body segments are in motion. The evaluation aims to detect whether the amplitude of these movements is excessive or reduced.
Body rhythm is the sum of the three aforementioned elements and to evaluate whether the rhythm is expression of constraint or freedom, it is sufficient to ask the patient the progressive variation of the three parameters, observing the execution modes.
The "what" is walking and the system will deploy all necessary strategies to achieve the goal; the "how" will provide useful information on the adaptations the system is forced to use.
Specific parameters
Referring to what should be physiological movement, strategies implemented by the individual patient will be observed.
* Skull: it should be free to orient itself in space and free from walking mechanisms.
* Shoulder girdle: it should have rotational movement for anteropulsion. The driving muscle of the action: pectoralis major.
* Upper limbs: should have an inertial pendular movement, without active muscular component.
* Pelvic girdle: should have a rotational movement for anteropulsion in counter-rotation with respect to the shoulder girdle. Responsible muscle for the action: rectus femoris.
* Lower limbs: when both feet are in support, the pelvis should be at the apex of an isosceles triangle, made up of the lower limbs as legs and the distance between the two feet as base. The step should have both an anterior and posterior moment. During the swing phase, the knee extension should initially be inertial and require the action of the quadriceps to complete the extension shortly before the foot reaches the support.
* Support base: during walking the heel center should lie along a vertical line passing through the ASIS, anterior-superior iliac spine, and the knee center.
* Foot: the reference is a line joining the center of the heel to the second toe. According to the statistical model (which considers physiological and normal the behavior of the majority), this line should diverge about 10 degrees; according to the engineering model (which considers the best possible performance based on structure), this line should be oriented forward.
Standing position
In standing position a dynamic evaluation will be carried out by asking the patient to actively correct skeletal elements (derotation of femurs, humeri, head position, etc.) observing overall skeletal adaptations and muscular execution modes.
Supine position
Dynamic observations will be divided into active, performed by the patient, and passive, performed by the operator.
Active dynamic observations
Aimed at detecting substitution muscle actions and incongruous skeletal movements. They concern:
* Active inspiratory phase: the chest should expand harmoniously in the 3 directions of space (cranially, anteroposteriorly and laterolaterally); the "belly" (hypogastric fascia) should be "inflated" passively as a consequence of pressure exerted by the diaphragm on the viscera, therefore in much reduced quantity and at a time subsequent to thoracic expansion. The case in which the hypogastrium anticipates thoracic movement with active modality, can be the signal of simultaneous activation of the pillars of the diaphragm and iliopsoas which, to facilitate thoracic expansion, exert a pulling force on the lumbar vertebrae. This type of inspiratory strategy, over time, can cause mechanical conflicts on lumbar vertebrae, also considering that the pillars of the diaphragm have asymmetric vertebral insertion (L1-L3 on the left, L1-L4 on the right) and that the traction on vertebral bodies also has a rotational component.
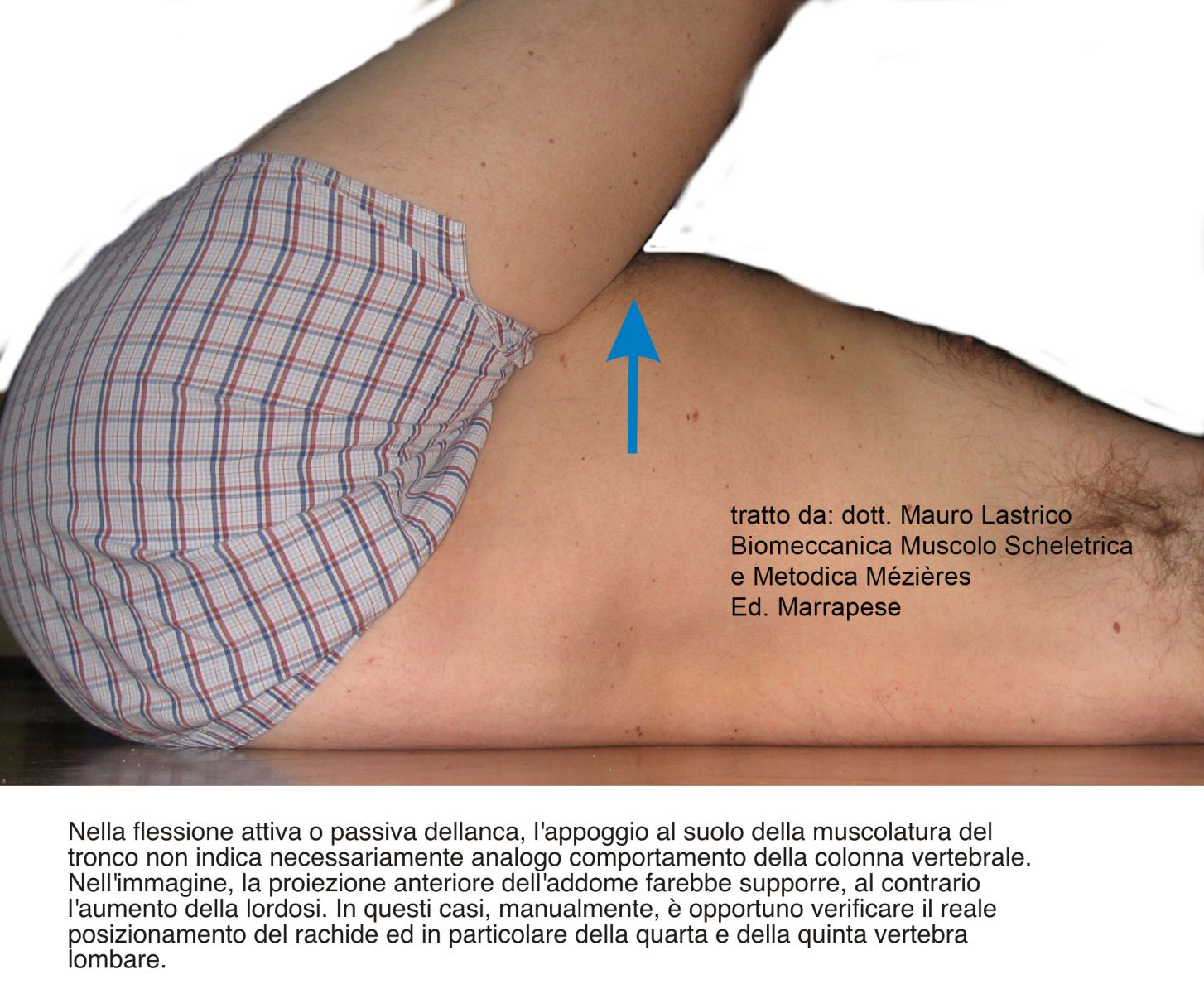
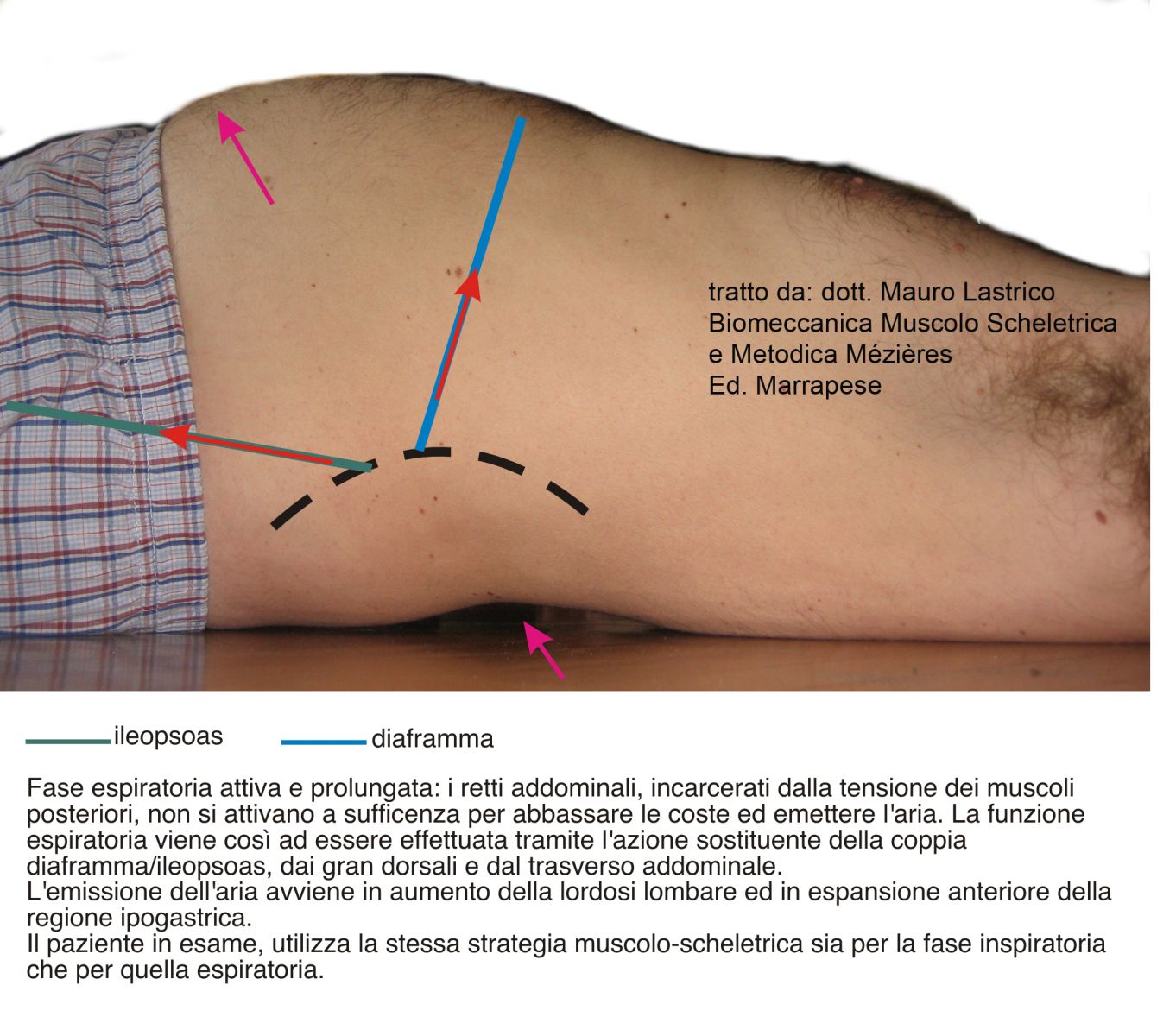
* Active and prolonged expiratory phase: the chest should descend towards the pelvis due to the action of the rectus abdominis and approach the midline due to the action of the oblique and transverse abdominal muscles. The lumbar vertebrae approach the floor. Also in this case the hypogastric fascia should not be projected anteriorly. If this happens it can be the signal of activation of the latissimus dorsi partially or totally substituting the rectus abdominis: the thoracic walls close excessively towards the midline and the chest descends insufficiently towards the pelvis, while the lumbar vertebrae (especially the fourth and fifth) sink. When there is substitution of the recti abdominis by the latissimus dorsi, detecting the movement of the lumbar vertebrae is particularly important, as often a descent of the first (L1 L2 L3) and a sinking of the last (L4 L5) is observed, with a consequent potential mechanical conflict between two adjacent vertebrae.

* Anteposition of the shoulders: the scapulae should move away from the spine and the latter move toward the floor, the sternoclavicular joint should act as a pivot and the driving muscle of the action should be the pectoralis major. In the event that the action of the pectoralis major is replaced using emergent abilities potentially possible for complex systems, the skeletal movement will be pathologic. In particular, if the substituting muscles are the latissimus dorsi and the upper trapezius bundle, the scapula will be hypomobile and the chest will participate in rotation, the first dorsal vertebrae will not move toward the floor, and the clavicle head will be projected anteriorly in subluxation or dislocation of the sternoclavicular joint.
Passive dynamic observations
Actions performed passively by the operator and aimed at verifying respect or not of physiology of skeletal reactions, muscle length state and joint freedom, both skeletal and muscular.
A list of some passive investigations follows. According to the specific problem of the patient, all those deemed appropriate for the functional evaluation of the case will be added.
In the description of muscles placed in passive elongation only the most vectorially significant muscles will be cited.
* Lateral inclination of the skull: skeletally the cervico-dorsal vertebrae should move with contralateral convexity and the chest should expand laterally contralaterally. The muscles placed in passive elongation are all the contralateral cranio-cervico-scapular and, if shortened, will modify the position of the scapula, clavicle and hyoid bone.
* Rotation of the skull: the cervico-thoracic vertebrae should rotate ipsilaterally and the chest should expand laterally contralaterally. The muscles placed in passive elongation are all the ipsilateral cranio-cervico-dorsal and, if shortened, will modify the position of the scapula, clavicle and hyoid bone.
* Abduction of the upper limbs: up to 80/90 degrees the humeral movement should occur within the glenoid cavity without causing skeletal movements. Beyond these degrees it is physiological that the chest expands laterally bilaterally and that the scapulae tilt adducing the superomedial angle and abducting the inferior angle. From 120 degrees forward the muscles placed in passive elongation are the humeral intrarotators. If shortened, they can cause: increased dorso-lumbar lordosis (latissimus dorsi), scapulae losing cohesion with the rib cage (subscapularis, teres major and scapulohumeral portion of latissimus dorsi, dominant over serratus anterior and scapular adductors); subluxation of the humerus.

* Elevation of the upper limbs: up to 60 degrees humeral movement should occur within the glenoid cavity without causing skeletal movements. Beyond these degrees, it is physiological: that the chest expands anteroposteriorly increasing dorso-lumbar lordosis; that the scapulae abduct parallelly putting the scapular adductors in passive elongation; that the upper dorsal vertebrae with apex at D5 go into kyphosis; that cervical-dorsal lordosis decreases due to relaxation of muscles placed anterior to the spine. Besides scapular adductors, the muscles placed in passive elongation are the humeral intrarotators. If shortened they can cause: excessive increase of dorso-lumbar lordosis (latissimus dorsi); scapulae losing cohesion with the rib cage (subscapularis, teres major and scapulohumeral portion of latissimus dorsi, dominant over serratus anterior and scapular adductors); subluxation of the humerus.
* Unilateral elevation of the lower limb: up to about 40/45 degrees femoral movement should occur within the hip joint without causing skeletal movements. Beyond these degrees, there is a slight rise of the ipsilateral hemipelvis, contralateral rotation of the hemipelvis and contralateral thoracic lateral expansion.
* Elevation of the lower limbs: adaptation analysis will be performed, if possible, by placing the lower limbs directly at 90 degrees. In this position the lower limbs should be extended and free of rotations, the pelvis supported on the ground in a neutral position, the thoraco-pubic line straight. Among the many adaptations that will actually occur, particular importance is assumed by the potential conflict between the pelvis, if retroverted, and the last lumbar vertebrae, if pulled anteriorly.
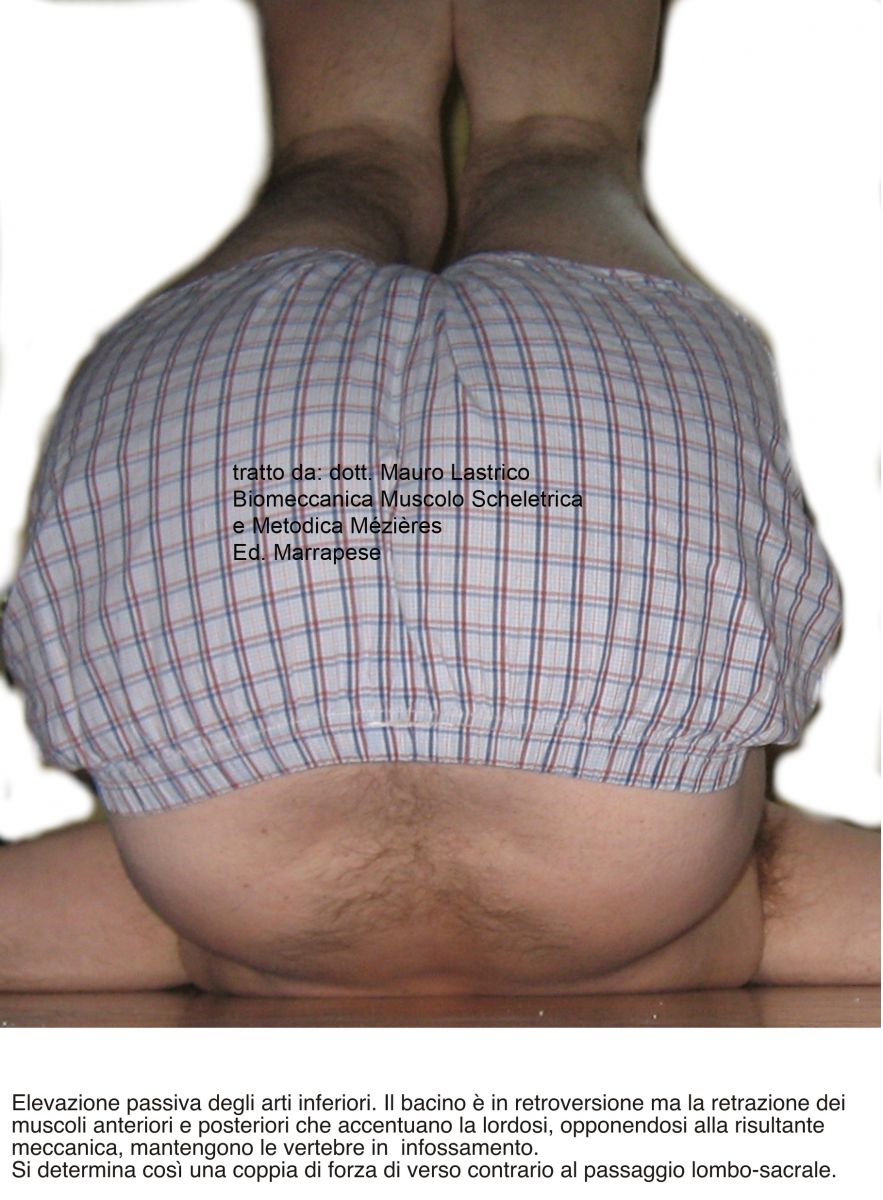
All passive or active actions that induce pelvic retroversion have in themselves a high danger index: in retroversion the pelvis causes a mechanical push on the lumbar vertebrae in the direction of delordosis but, if at the same time act, with varying degrees of intensity and synergy, latissimus dorsi, quadratus lumborum, paravertebrals, diaphragm and iliopsoas, muscles that increase lumbar lordosis, a couple of opposing forces will be produced that can create mechanical conflicts up to true listhesis, at the lumbosacral junction.
In hip flexion actions it is therefore important to differentiate between the position of muscles and that of vertebrae: the support on the ground of the trunk musculature does not necessarily imply analogous behavior of the spine.