AIFiM M
Italian Association of Physiotherapists for the Study and Development of the Mezieres Method
Advanced Institute of Neuro-Myo-Fascial Biomechanics
AIFiMM Provider ECM n° 1701
The only Mezieres school to have been directly recognized by the Italian Ministry of Health, becoming ECM Provider n° 1701


Biomechanics of Muscle Shortening Causes
Dr. Mauro Lastrico
Biomechanics: causes of muscle shortening
Dr. Mauro Lastrico, physiotherapist.
ABSTRACT
This article proposes a physical interpretation of muscle shortening phenomena based on material mechanics principles. Starting from the clinical observation that muscles tend to shorten their length, we apply the theory of differential elasticity coefficients to explain how contractile components (high elastic coefficient) and connective components (low elastic coefficient) respond differently to mechanical stress.
The model introduces the fundamental concept of the inversely proportional relationship between Resistive Force (RF) and Work Force (WF), demonstrating how connective component shortening generates mechanical inefficiency rather than true muscle weakness. The cart-with-brake analogy illustrates how muscle maintains its force-generating capacity but dissipates it internally to overcome its own structural resistances.
Model implications include static alterations (joint axis modifications), dynamic changes (increased energy expenditure), and the tendency toward perpetuation through adaptive compensations. Shortening reversibility is predicted by the same physical laws through application of appropriate forces for times compatible with tissue viscoelastic properties.
This approach, valid in the absence of specific pathologies, offers a rigorous and verifiable interpretive framework for musculoskeletal phenomena commonly observed in clinical practice.
Keywords: muscle mechanics, elasticity coefficient, resistive force, work force, connective shortening
1 Clinical Observation of Muscle Shortening
Clinical practice reveals a phenomenon: muscles tend to shorten their length. This empirical observation occurs systematically in the absence of specific congenital or acquired pathologies, neurological or otherwise.
The muscle, while maintaining contractile capacity, may present a reduced baseline length that alters joint geometry and limits movement excursion. This condition poses a question: what physical interpretation can explain this phenomenon?
2 Physical Laws of Elastic Deformation
If we accept that the human body follows the same universal physical laws, material mechanics provides the interpretive key to the phenomenon.
From materials physics, we know that any body subjected to deforming forces undergoes modifications based on its elasticity coefficient. The ideal elasticity coefficient equals 1: representing a perfectly elastic material that completely returns accumulated energy, returning exactly to its initial state. In nature, such materials do not exist.
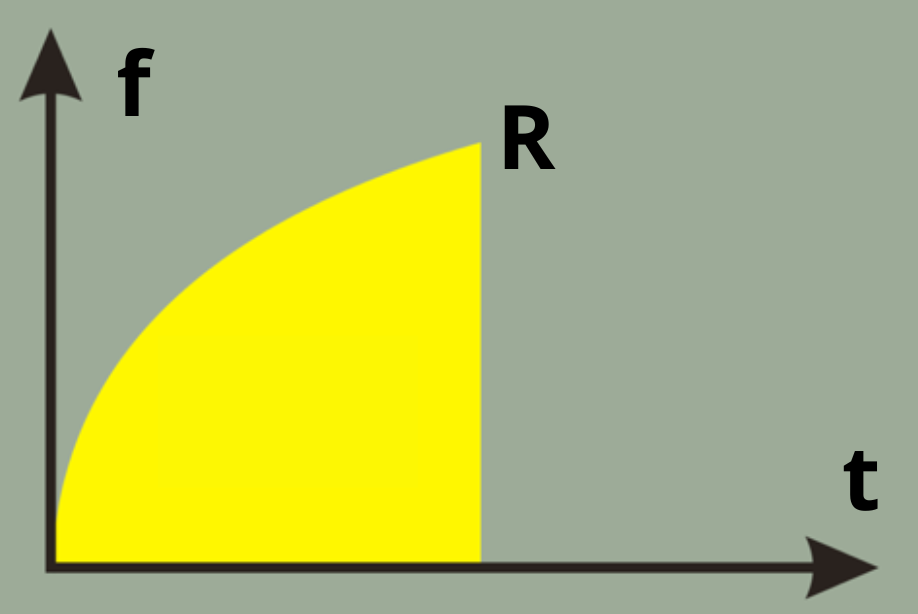
fig. 01
- f: force
- t: time
- R: breaking load
- yellow: energy return area curve of elastic materials: coefficient of elasticity E = 1
Real materials have coefficients less than 1 and maintain residual deformations proportional to applied force and application time. The greater the force-time product, the greater the potential permanent deformation.
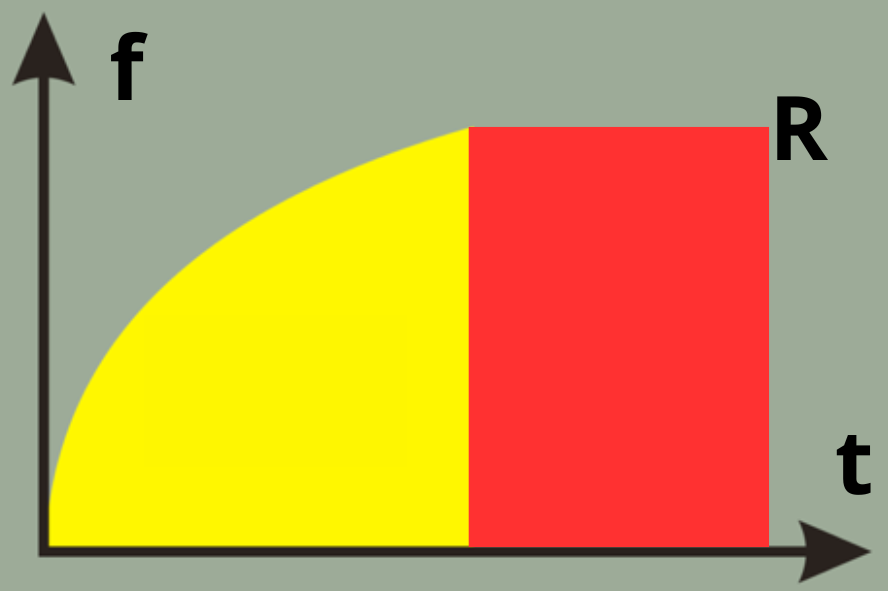
fig. 2
- f: force
- t: time
- R: breaking load
- yellow: energy return area
- red: area of permanent deformations curve of plastic materials: coefficient of elasticity E < 1
3 Application of Physical Laws to Muscle Tissue
Muscle tissue is composed of materials with different elasticity coefficients:
Contractile components (actin and myosin): present high elasticity coefficient, close to ideal. After contraction, they tend to return to original length. Their alteration manifests primarily as baseline tone variation.
Connective components (endomysium, perimysium, epimysium, tendons): present lower elasticity coefficient. Subjected to prolonged compressive forces, they can maintain residual deformations.
This difference in elastic behavior is clinically observable: muscle relaxation techniques effectively act on tone (contractile components) but have limited effect on structural connective tissue shortening.
4 Mechanical Classification of Elastic Elements
From a mechanical perspective, muscle elastic elements behave in two modalities:
Series elastic elements (tendons and their extensions): cushion stress during contraction, protect muscle from injury, return accumulated elastic energy. They generally do not undergo significant modifications during normal muscle activity.
Parallel elastic elements (intramuscular connective tissue): undergo direct compression during muscle contraction, can maintain residual deformations proportional to applied force-time product, represent the principal site where muscle shortening is hypothesized to occur.
5 Physical-Mathematical Model of Muscle Fiber
Representing muscle behavior according to a mathematical model based on physical laws:
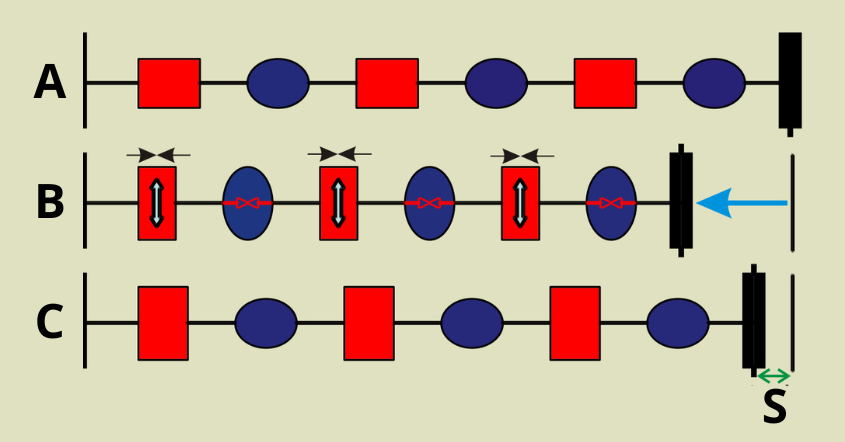
fig. 3
- A: muscle fiber at rest
- B: contraction
- C: relaxation
- S: sum of residual muscle shortening
- red: connective portions
- blue: contractile portions
- black vertical lines: muscle insertions
During contraction (B), contractile components generate traction bringing insertions closer. This determines compression of parallel connective components. Upon relaxation (C), contractile components tend to return to initial length due to their high elastic coefficient, while connective components may maintain residual deformation (S) proportional to the contraction force-time product.
Progressive shortening hypothesis: The summation of residual deformations in connective components could explain the progressive muscle shortening observed clinically. This process would be cumulative over time.
6 Fundamental Mechanical Principle: Muscle Generates Only Traction
Muscle can exclusively generate traction force by bringing its insertions closer. It cannot push or actively move insertions apart. This mechanical principle, always valid in the absence of specific pathologies, has important consequences:
- Shortened muscles maintain constant traction on insertions
- The skeleton has no autonomous movement capacity
- Skeletal axis alterations are consequences of muscle forces
7 Connective Shortening and Skeletal Alterations
If connective components shorten according to the proposed model, the muscle would maintain reduced length even at rest. This mechanical condition could determine skeletal adaptations according to the following modalities:
- Muscle insertions are brought closer by passive tension of shortened connective tissue
- Joints modify their axes to accommodate new muscle length
- Physiological joint sequence is altered in a predictable manner according to vector analysis
This mechanism, always considering the absence of specific pathologies, explains alterations of the physiological joint sequence observable clinically. The skeleton passively adapts to muscle forces according to mechanical laws.
8 Resistive Force and Work Force: Interpretation of Dynamics
Connective component shortening affects not only statics but alters muscle dynamics through the relationship between Resistive Force and Work Force.
Resistive Force (RF): passive tension generated by shortened connective tissue. Represents the structural internal resistance that muscle must overcome before producing movement.
Work Force (WF): force quota available to generate useful movement after overcoming internal resistances.
Physical relationship: RF and WF are inversely proportional. As Resistive Force increases, available Work Force proportionally decreases.
A muscle with shortened connective components must dissipate energy to overcome its internal rigidity before producing movement. It's like pushing a cart with the parking brake engaged: the motor (contractile component) works perfectly but much of the energy is dissipated overcoming friction (shortened connective component).
This physical principle explains why a shortened muscle appears "weak" when in reality it maintains intact force-generating capacity. It's not weakness: it's mechanical inefficiency due to increased Resistive Force.
9 Verifiability of the Proposed Model
The model based on elastic deformation laws finds support in several clinical observations:
- Muscle length tests: reveal measurable shortening
- Differential response to treatments: relaxation techniques effectively act on tone (high elastic coefficient contractile components) but have limited or no effect on structural connective shortening (low elastic coefficient)
- Recovery times: muscle length recovery requires times compatible with plastic material remodeling
- Recurring patterns: shortening follows vectorially analyzable force lines
These observations, while not constituting definitive proof, are consistent with the proposed physical model.
10 Shortening Reversibility
The same physical laws that determine shortening predict its reversibility. As a plastic material can be remodeled by applying appropriate forces for adequate times, so connective muscle tissue can recover length.
Reversibility requires application of specific therapeutic techniques for times compatible with the treated material's viscoelastic properties.
11 Systemic Implications
Connective component shortening generates the following consequences:
Static alterations:
- Modification of joint axes through mechanical adaptation
- Altered load distribution on joint surfaces
- Asymmetric stress on joint structures
Dynamic alterations:
- Joint excursion limitation due to mechanical constraint
- Increased energy expenditure to overcome internal resistances
- Movement pattern modification
Phenomenon perpetuation:
- Altered patterns generate further compensatory shortening
- The nervous system normalizes alterations, interpreting them as new baseline condition
- A circuit of alteration maintenance and amplification is established
These consequences, always in the absence of specific pathologies, derive directly from applying physical laws to the musculoskeletal system.
Summary of Proposed Concepts
Clinical observation reveals that muscles present shortening, in the absence of specific pathologies.
Physical interpretation through elastic deformation laws explains the phenomenon via different tissue elasticity coefficients.
Selective shortening predominantly affects connective components compared to contractile ones.
Static consequences: shortened muscles determine skeletal adaptations according to mechanical laws.
Dynamic consequences: increased Resistive Force reduces available Work Force, creating mechanical inefficiency.
Reversibility is possible through application of specific therapeutic techniques based on the same physical principles.
This interpretive model, based on physical principles and clinical observations, offers a coherent explanation of phenomena observed in the absence of specific pathologies.
This article is part of the scientific framework developed in the online course Systemic Musculoskeletal Biomechanics (CPD Certified – UK, CEU Approved – USA).
👉 https://aifimm.it/en/cc/systemic-musculoskeletal-biomechanics
Copyright © 2025 AIFiMM Formazione Mézières Provider E.C.M. n. 1701. All rights reserved.