AIFiM M
Italian Association of Physiotherapists for the Study and Development of the Mezieres Method
Advanced Institute of Neuro-Myo-Fascial Biomechanics
AIFiMM Provider ECM n° 1701
The only Mezieres school to have been directly recognized by the Italian Ministry of Health, becoming ECM Provider n° 1701


Biomechanics of the Spine: Frontal and Rotatory Planes. Scoliosis
Dr. Mauro Lastrico
Biomechanics of the spine in the frontal and rotational planes. Scoliosis
Dr. PT Mauro Lastrico
Excerpt from:
"Musculoskeletal Biomechanics and the Mézières Method"
Author: Dr. Mauro Lastrico
Marrapese Publisher
INTRODUCTORY NOTE:
Vertebral body rotation (which, by anatomical convention, refers to the posterior aspect) causes lateral displacement of the vertebrae relative to the midline, producing a contralateral vertebral convexity.
Since rotation and convexity are mechanically linked, throughout the following article only the convexity will be indicated, with the understanding that vertebral body rotation occurs in the opposite direction.
This “rule” of vertebral behavior does not apply in certain types of scoliosis, where rotation and convexity may occasionally occur on the same side.
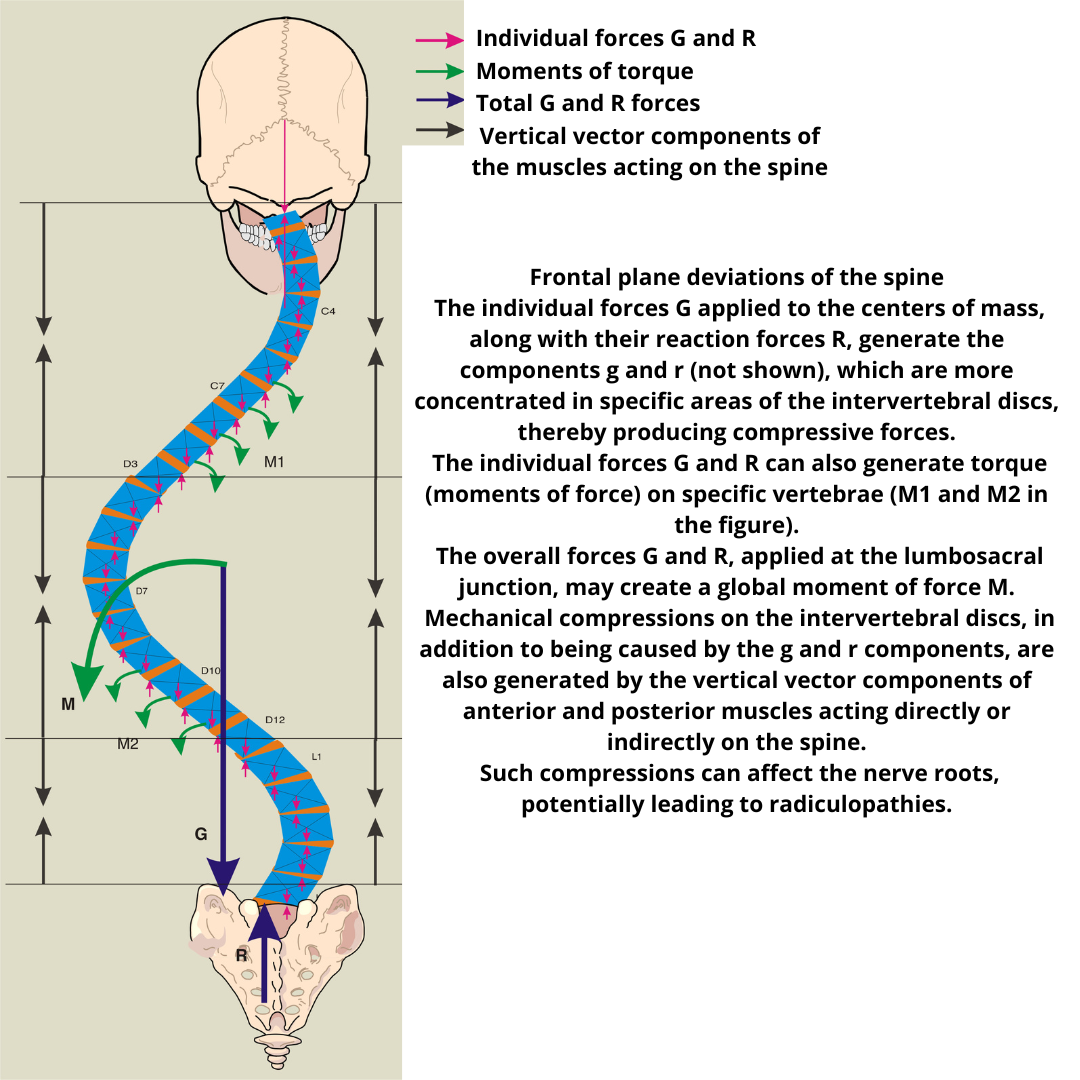
In the lateral deviations of the spine, similarly to what occurs in the sagittal plane, the G and R forces applied to each individual center of gravity can cause focused and asymmetric compressions on the intervertebral discs and moments of force.
The overall G and R forces, applied at the lumbosacral junction, can produce significant compressions on the disc as well as an overall moment of force.
The compressive forces on the intervertebral discs are also determined and accentuated by the vertical vector components of all muscles, both anterior and posterior, acting directly or indirectly on the spine.
These compressions can eventually affect the roots of the plexuses, leading to radiculopathies.
Latissimus Dorsi Patterns
Having numerous insertion points, the shortening of this muscle produces various skeletal effects.
Schematically, two main patterns can be distinguished: "A" and "B".
These patterns are not always "pure" and mixed patterns are often observed.
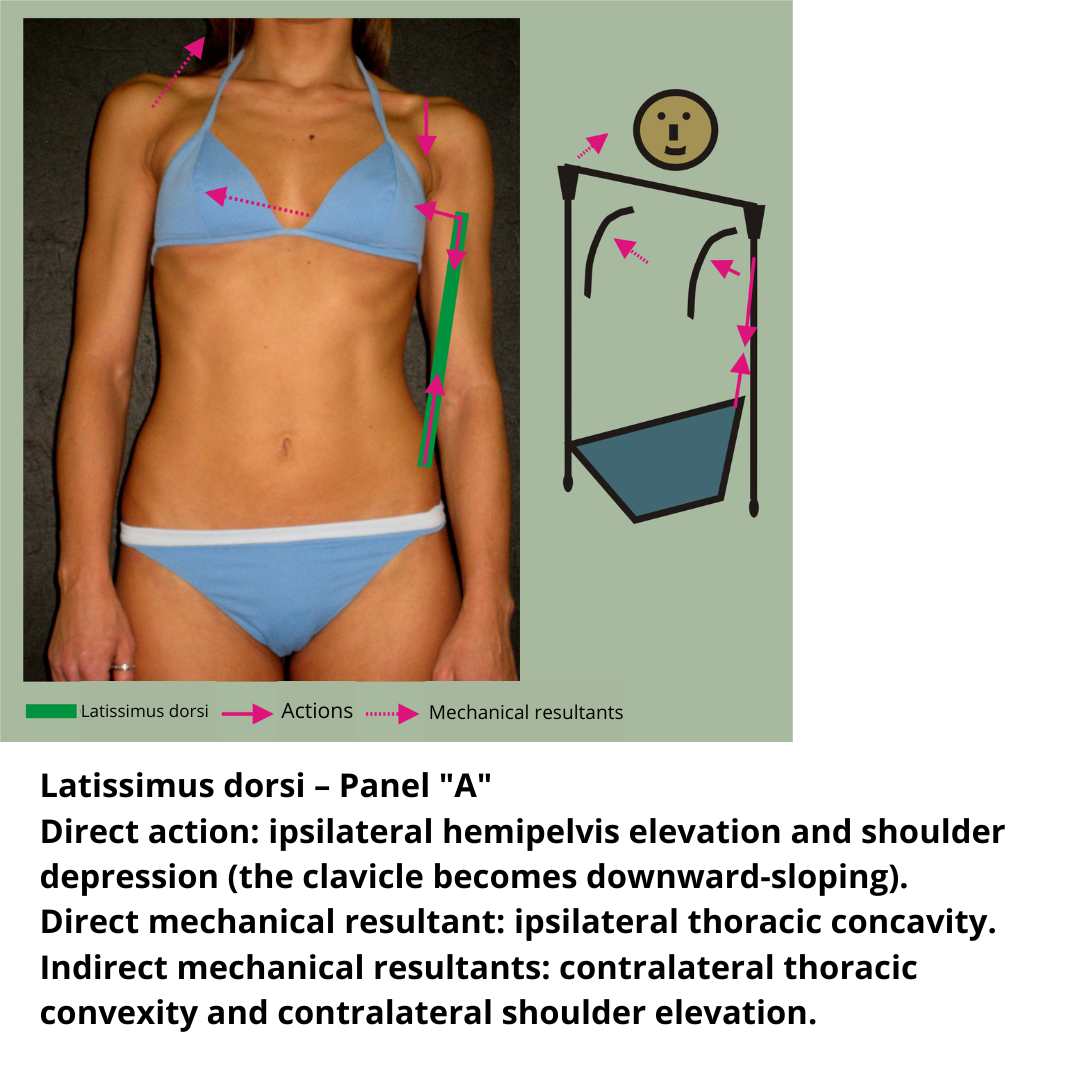
* Pattern "A"
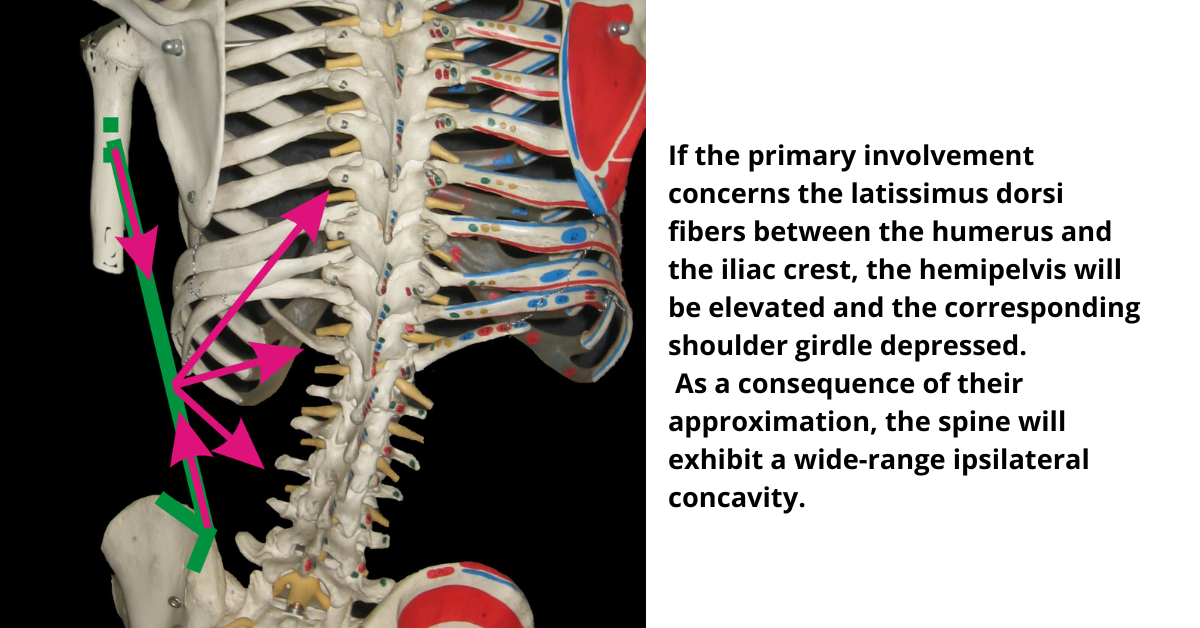
In this pattern, primarily the bundles of the latissimus dorsi that run from the iliac crest to the humerus are involved. By bringing the hemipelvis and the shoulder closer together, they cause a direct lowering of the shoulder and elevation of the hemipelvis, and as a mechanical result, the lateral concavity of the thoracic spine on the same side. These bundles are also responsible, due to mechanical results, for the contralateral convexity of the thoracic spine and the elevated contralateral shoulder.
If the mechanical result predominates, the spine will present a long-radius scoliosis with contralateral convexity, which is actually a consequence of the ipsilateral concavity caused by the approximation of the shoulder and the hemipelvis.
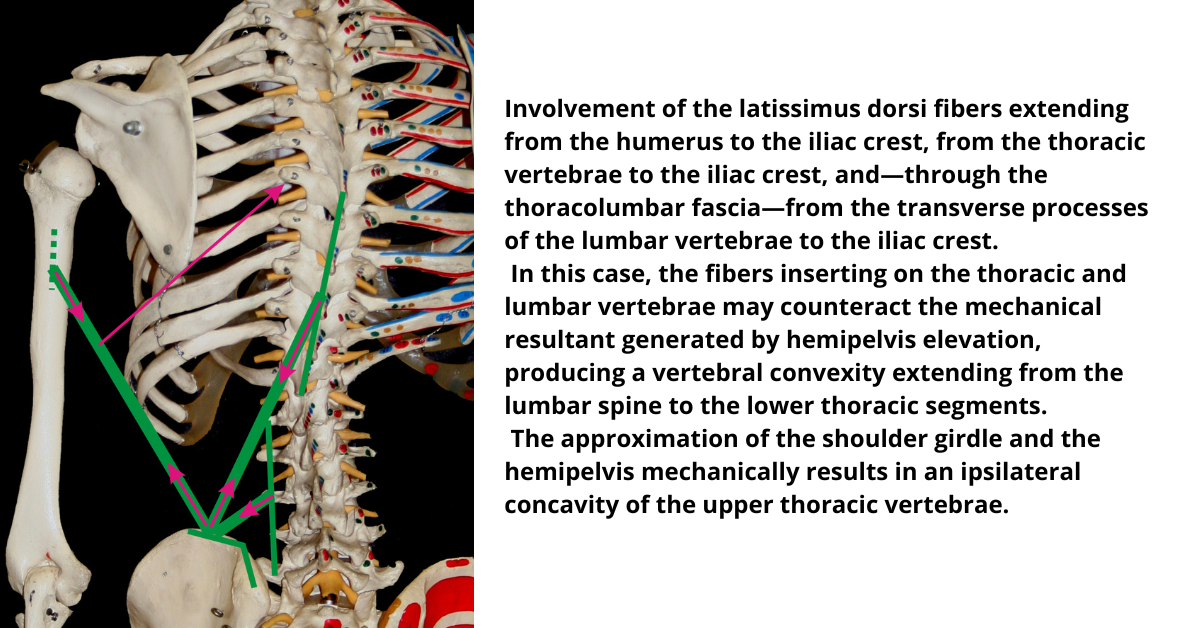
The latissimus dorsi has insertions on the spinous processes from T12 to T7 and, through the thoracolumbar fascia, on the costiform processes of the lumbar vertebrae. The quadratus lumborum, in addition to the twelfth rib, has insertions on the costiform processes of the first three lumbar vertebrae. Their line of force, therefore, is not only able to raise the hemipelvis but also to draw the vertebrae from L5 to T7.
The latissimus dorsi and the quadratus lumborum can oppose the mechanical result caused by the elevation of the hemipelvis, keeping the spine vertical or even creating an ipsilateral convexity.
In this case, a double curvature occurs, where the latissimus dorsi and the quadratus lumborum are directly responsible for the lumbar and lower thoracic vertebral convexity by direct traction on the vertebrae, and the upper thoracic concavity due to the approximation of the shoulder and the hemipelvis.
* Pattern "B"
This pattern is characterized by the combined action of the upper bundles of the latissimus dorsi and the muscles primarily responsible for elevating the shoulder girdle. Together, these muscles have a resultant force that causes adduction and elevation of the scapula and clavicle. If the omohyoid is also involved, the hyoid bone will be laterally deviated.
The thoraco-humeral bundles of the latissimus dorsi produce a lateral thoracic convexity in the lower quadrant, while the lower bundles raise the hemipelvis and rotate it backward.
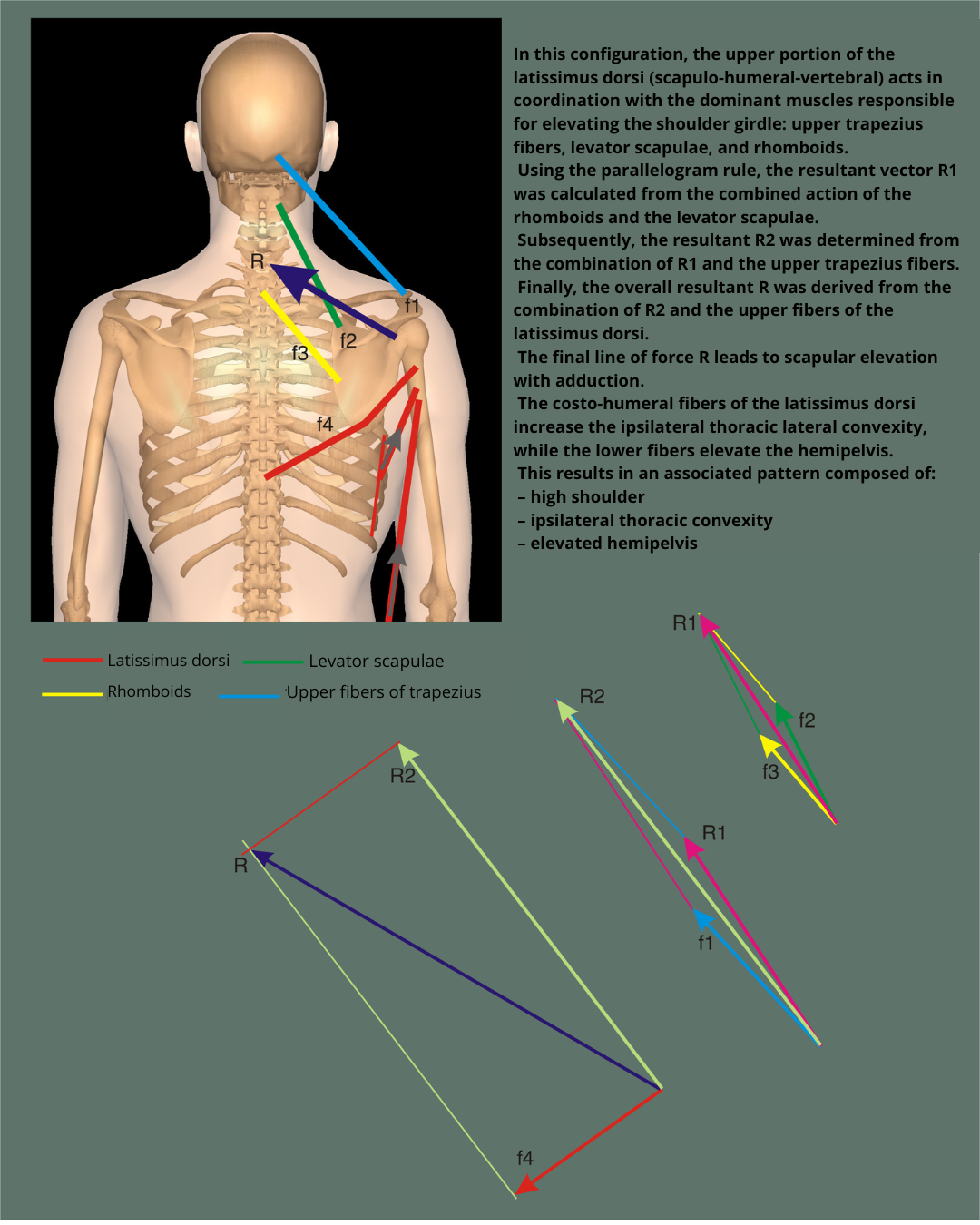
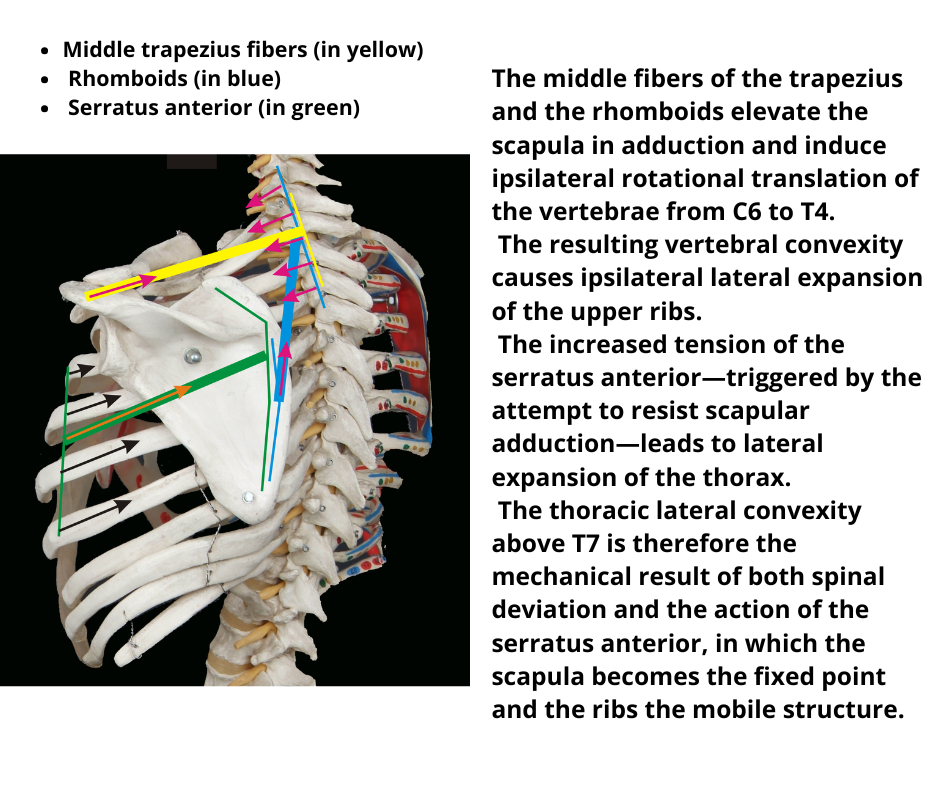
Moreover, the lateral thoracic convexity is also a mechanical consequence of the elevation of the shoulder girdle, which is directly caused by the rhomboids and the middle portions of the trapezius. These muscles, by elevating and adducting the scapula, can produce an ipsilateral convexity of the thoracic vertebrae. This convexity can extend into the upper lateral quadrant of the chest and, to further accentuate the distortion, the serratus anterior may also be engaged. The serratus, by trying to oppose the adduction and upward displacement of the scapula, has its insertion point fixed, and its line of force acts upon the ribs, causing them to shift laterally.
The combined pattern may potentially result in the following skeletal characteristics, although not necessarily all present, due to direct muscular action:
* Elevated and adducted scapula
* Ascending clavicle
* Lateral displacement of the hyoid bone
* Lateral thoracic convexity in the upper quadrant (above T7)
* Lateral thoracic convexity in the lower quadrant (below T7)
* Elevated hemipelvis
* Posterior rotation of the hemipelvis

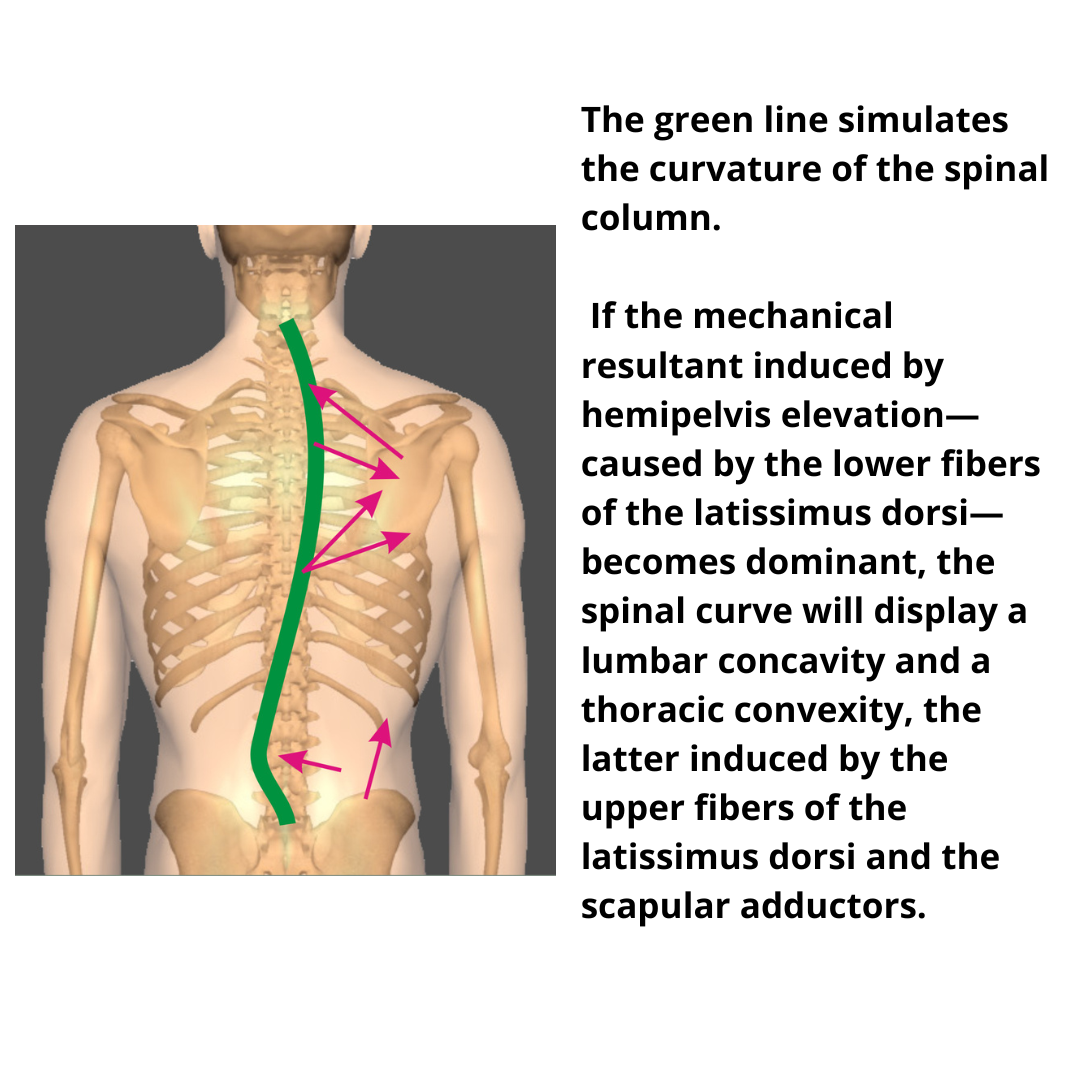
In the lumbar area, if the mechanical result caused by the elevation of the hemipelvis predominates over the vertebrae, it can lead to a double scoliotic curve, with lumbar concavity and thoracic convexity. The lower bundles of the latissimus dorsi elevate the hemipelvis, while the upper bundles, combined with the rhomboids and the middle and lower portions of the trapezius, determine the vertebral convexity of the thoracic spine.
In the case where the latissimus dorsi bundles that connect the pelvis and the thoracolumbar spine, together with the quadratus lumborum, are shortened, they counteract the mechanical result caused by the elevation of the hemipelvis. This allows the thoracolumbar spine to maintain a vertical or ipsilateral convex alignment.
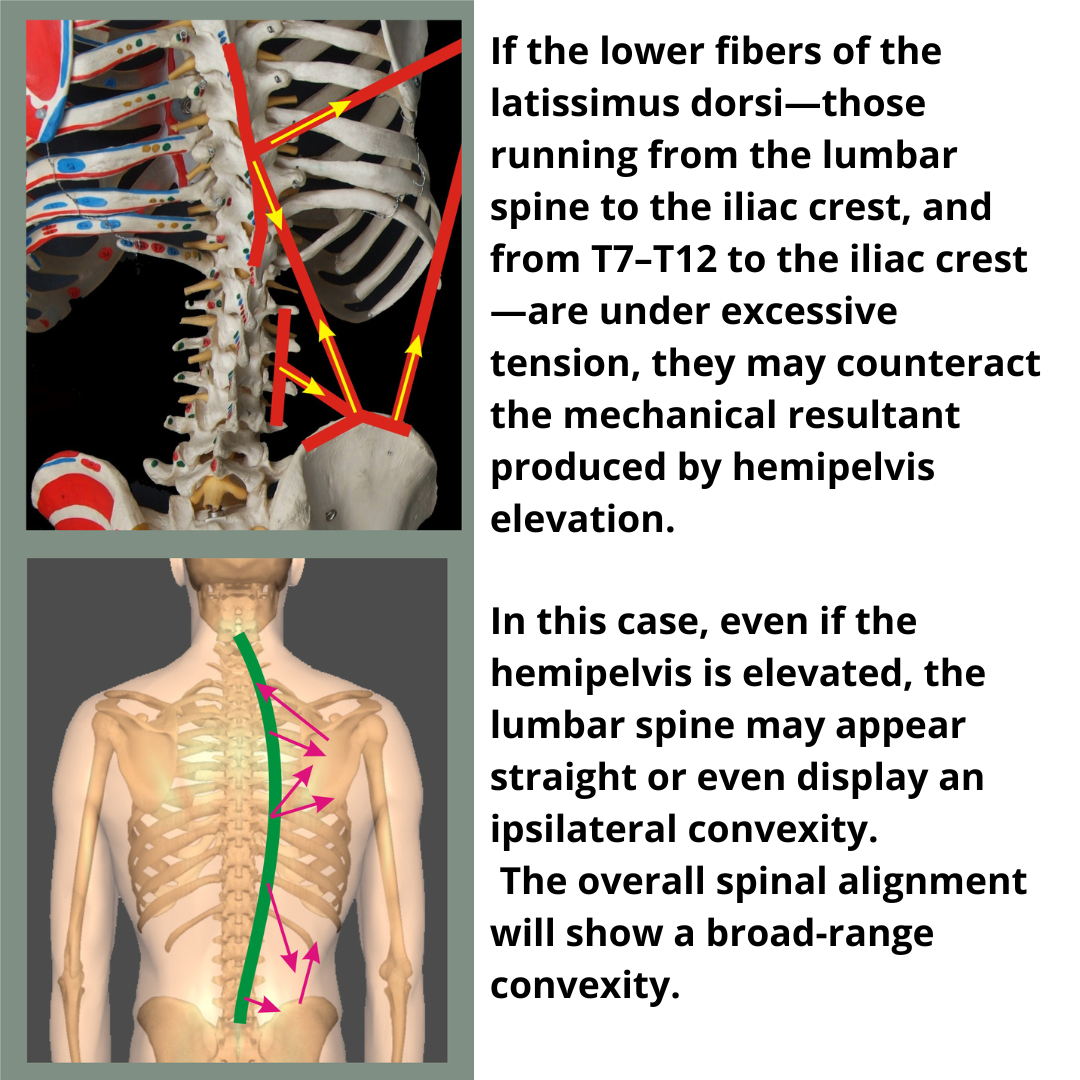
This results in a long-radius curvature where the thoracolumbar convexity is caused directly by the traction forces of the latissimus dorsi and the quadratus lumborum. Meanwhile, the upper thoracic convexity is induced by the adductors of the scapula and the mechanical result of the elevated shoulder.
Cranium
The position of the skull in space is ensured by postural reflexes through the cocontraction of all cranio-cervico-scapular muscles. Since a horizontal gaze is a dominant function, significant alterations due to cranial rotation or inclination are rare. It is more common for the underlying skeletal structures to adapt in order to allow a good positioning of the head. In this context, the hyoid bone plays a fundamental role due to its numerous connections.
If cranial rotation and inclination are observed as dominant elements, one should suspect the interference of disturbances arising from other systems, such as the visual (ocular suppression, strabismus, latent strabismus, ocular torticollis, etc.) or ENT (ear, nose, throat), making it important to carry out specific examinations in collaboration with specialists.
Cervical Vertebrae
Lateral displacement of the cervical vertebrae can be caused by direct or indirect muscular action.
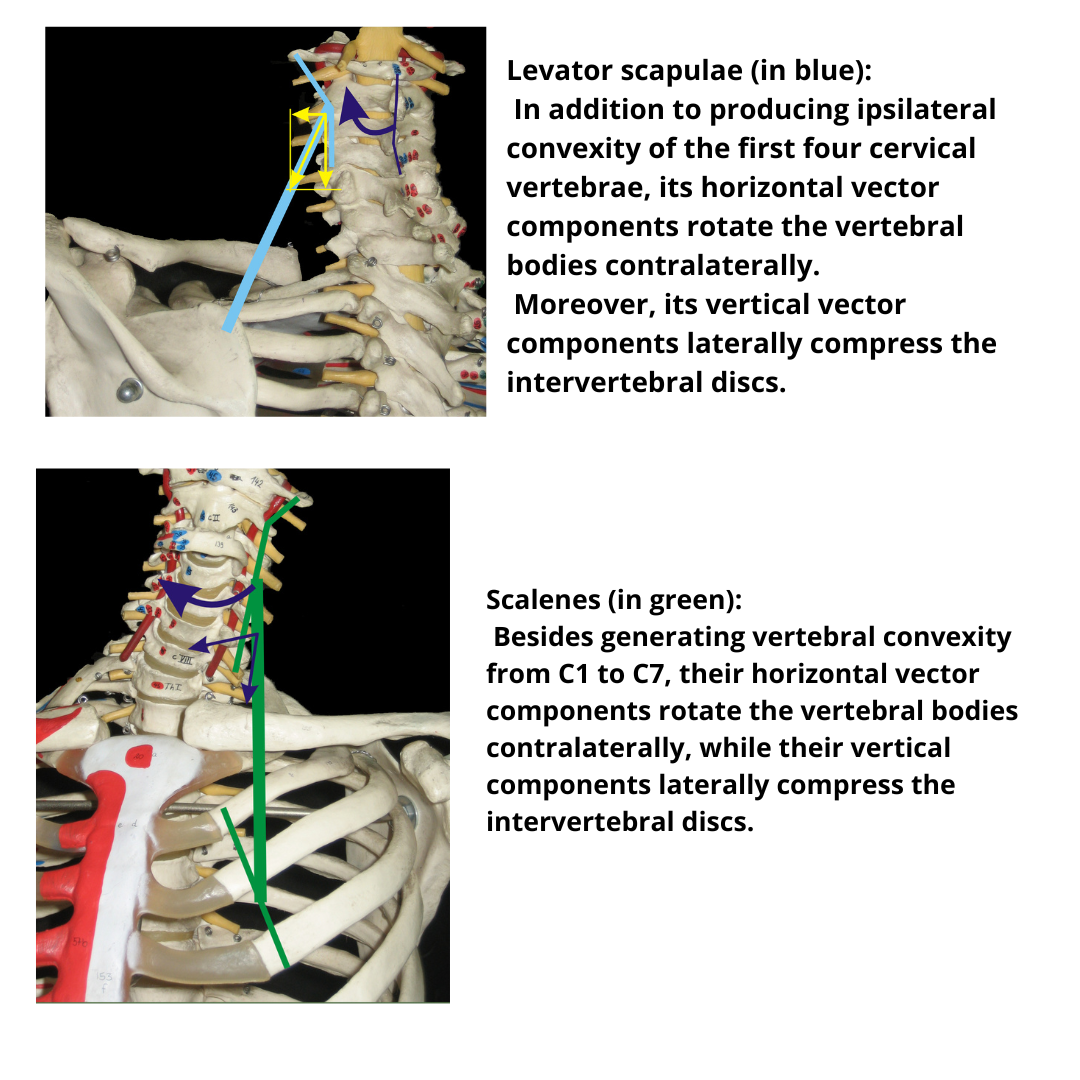
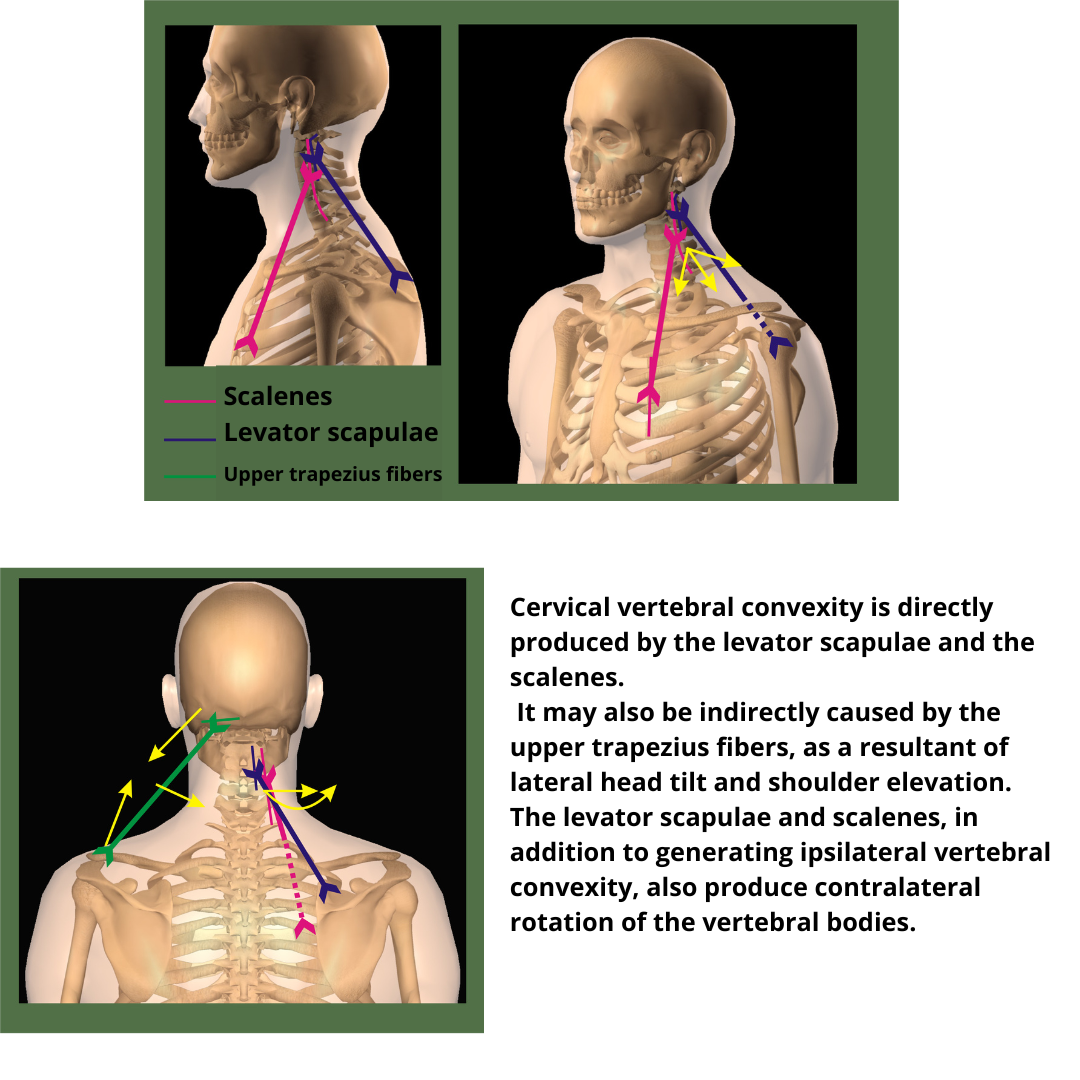
Direct action is performed by the levator scapulae and scalene muscles, with vertebral convexity occurring on the same side as the line of tension. In association with vertebral convexity, an elevated and adducted scapula (levator scapulae) and protrusion of the first ribs (scalene muscles) can also be observed.
Indirect action is caused by the upper bundle of the trapezius which, despite having no vertebral insertions, can cause a vertebral concavity on the same side due to the mechanical result of head tilt and scapular elevation.
Both the scalenes and the levator scapulae, through their horizontal vector components, cause contralateral vertebral body rotation, while their vertical vector components cause asymmetric compression of the intervertebral discs. This compression is exacerbated by the forces G and R acting upon each vertebra. When prolonged over time, such compressions can affect the roots of the plexuses, leading to radiculopathies.
Cervicothoracic Vertebrae (C6-T4)
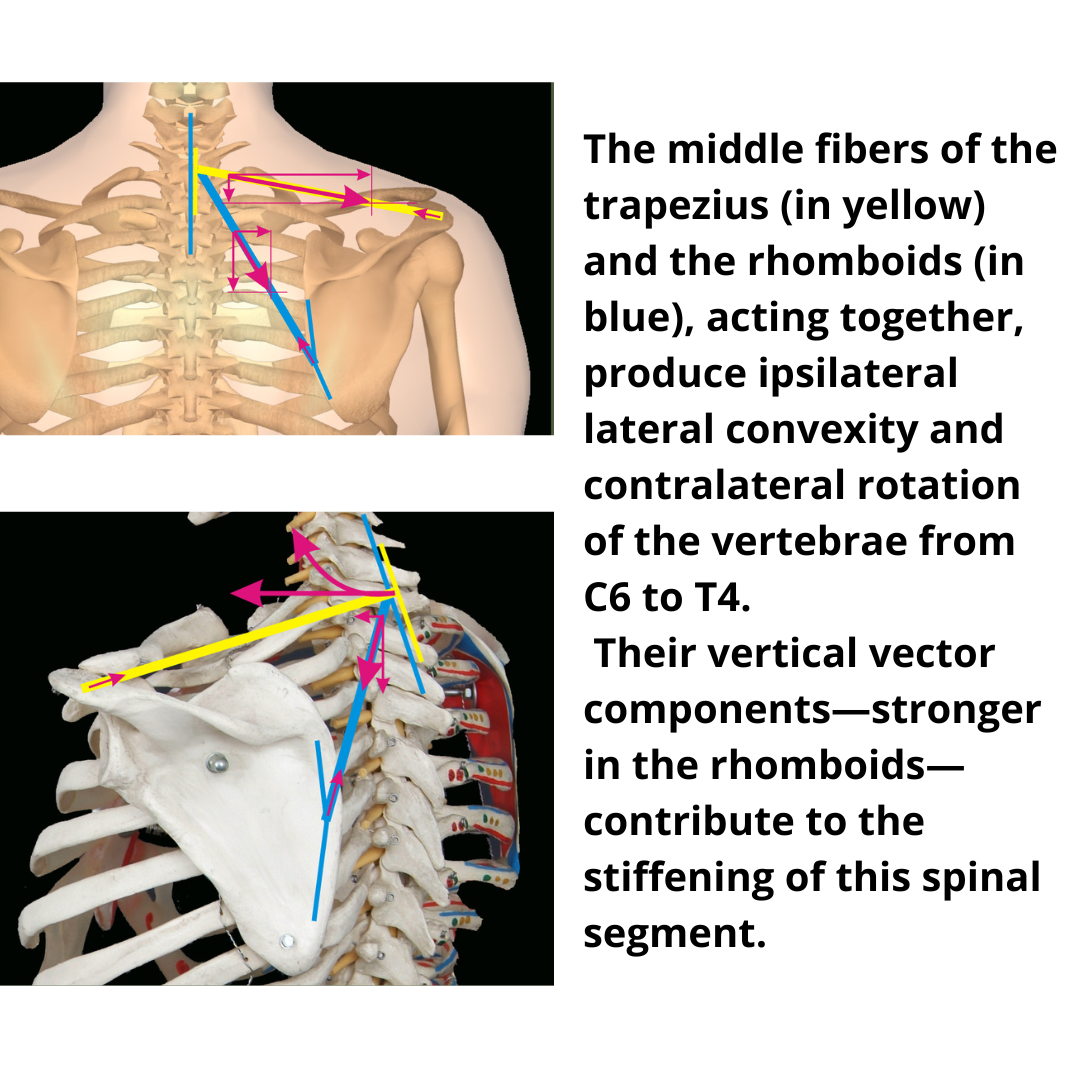
In this segment of the spine, direct action is exerted by the rhomboids (both major and minor) and the middle portions of the trapezius. In addition to causing vertebral convexity, these muscle groups rotate the vertebrae contralaterally.
Their longitudinal vector components, which are more prominently expressed by the rhomboids, stiffen the segment C6–T4.
These effects help maintain postural stability and define the dynamics of this area of the spine.
Thoracic Vertebrae (T2–T12)
Lateral displacement can be induced:
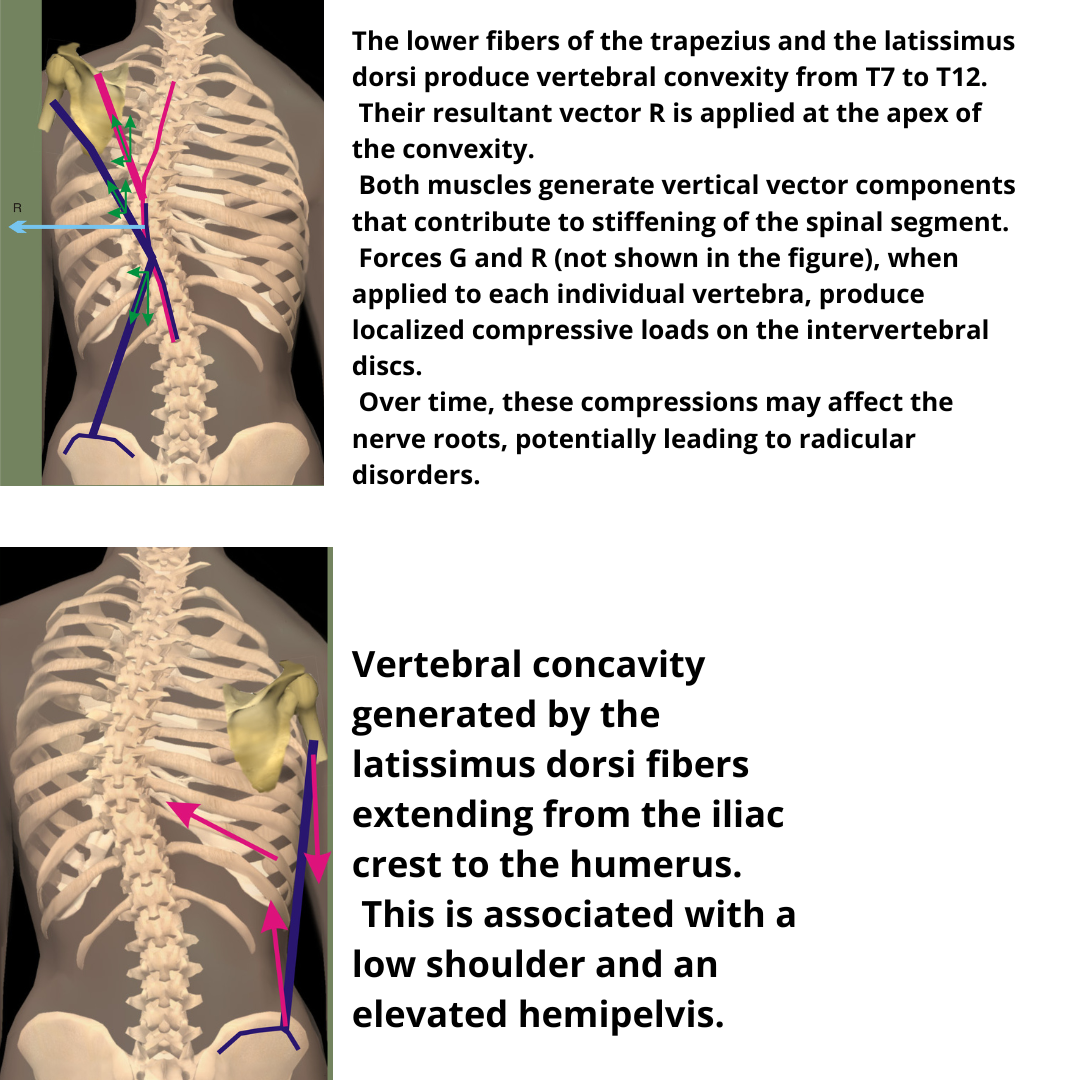
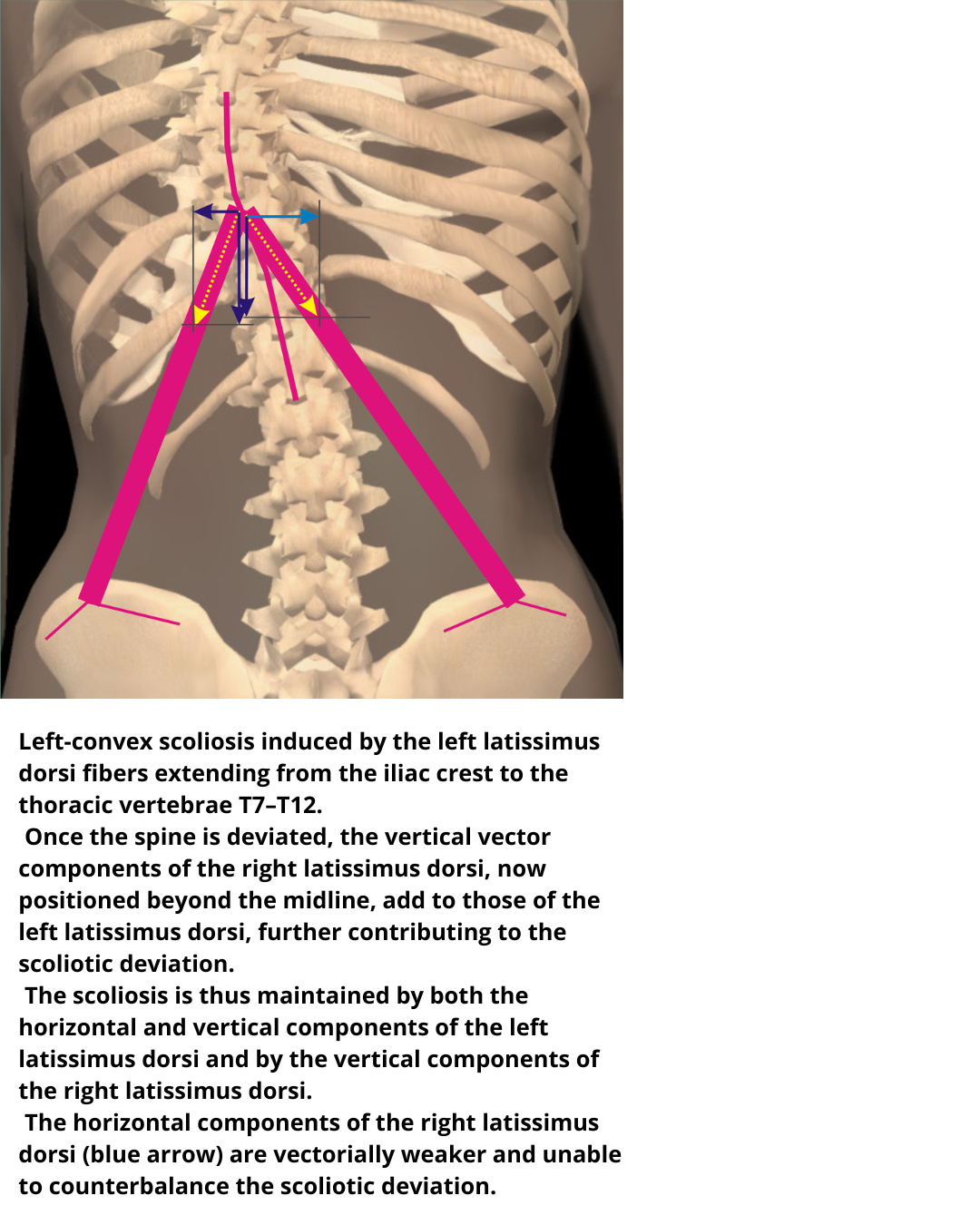
* Directly by the lower bundles of the trapezius and the portion of the latissimus dorsi extending between the thoracic vertebrae (T7–T12), the inferior angle of the scapula, and the humerus.
* By the portion of the latissimus dorsi extending between the thoracic vertebrae and the iliac crest.
The combined action of these muscle groups produces vertebral convexity with contralateral vertebral body rotation.
The vertical vector components of both muscles, combined with the paravertebrals, stiffen the spine.
The individual G and R forces applied to each vertebra, through their g and r components, cause localized and asymmetric compressive forces upon the intervertebral discs.
These compressions, if prolonged, can affect the root nerves, leading to radiculopathies.
Indirectly, lateral displacement can also be caused by the latissimus dorsi bundles that connect the humerus and the iliac crest. In this case, the action of the muscle produces concavity. As an associated pattern, the shoulder appears lower, and the hemipelvis appears elevated.
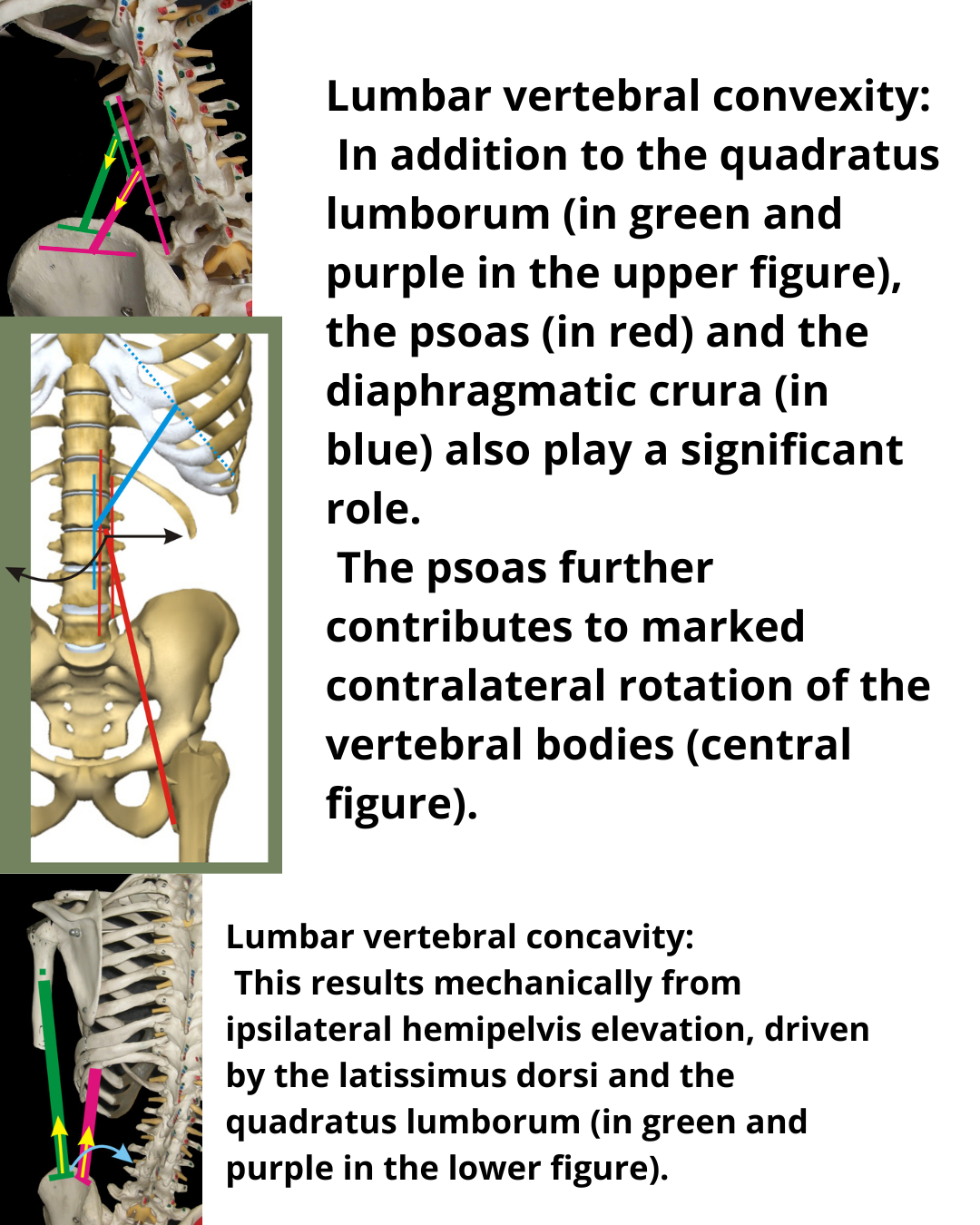
Lumbar Vertebrae
Lateral displacement is caused directly by the bundles of the latissimus dorsi inserted in the thoracolumbar fascia (L1–L5) and by the quadratus lumborum. Additionally, it is influenced by the diaphragm and the psoas muscles, which, through vertebral body rotation, contribute to the lateral displacement. In combined action, these muscles create an ipsilateral convexity.
Contralateral lateral displacement can also arise from the mechanical result caused by the elevation of the pelvis, due to the action of the latissimus dorsi and the quadratus lumborum when acting as a base of support.
Scoliosis
The etiology of scoliosis is still unknown. There are many hypotheses, including the psychosomatic theory.
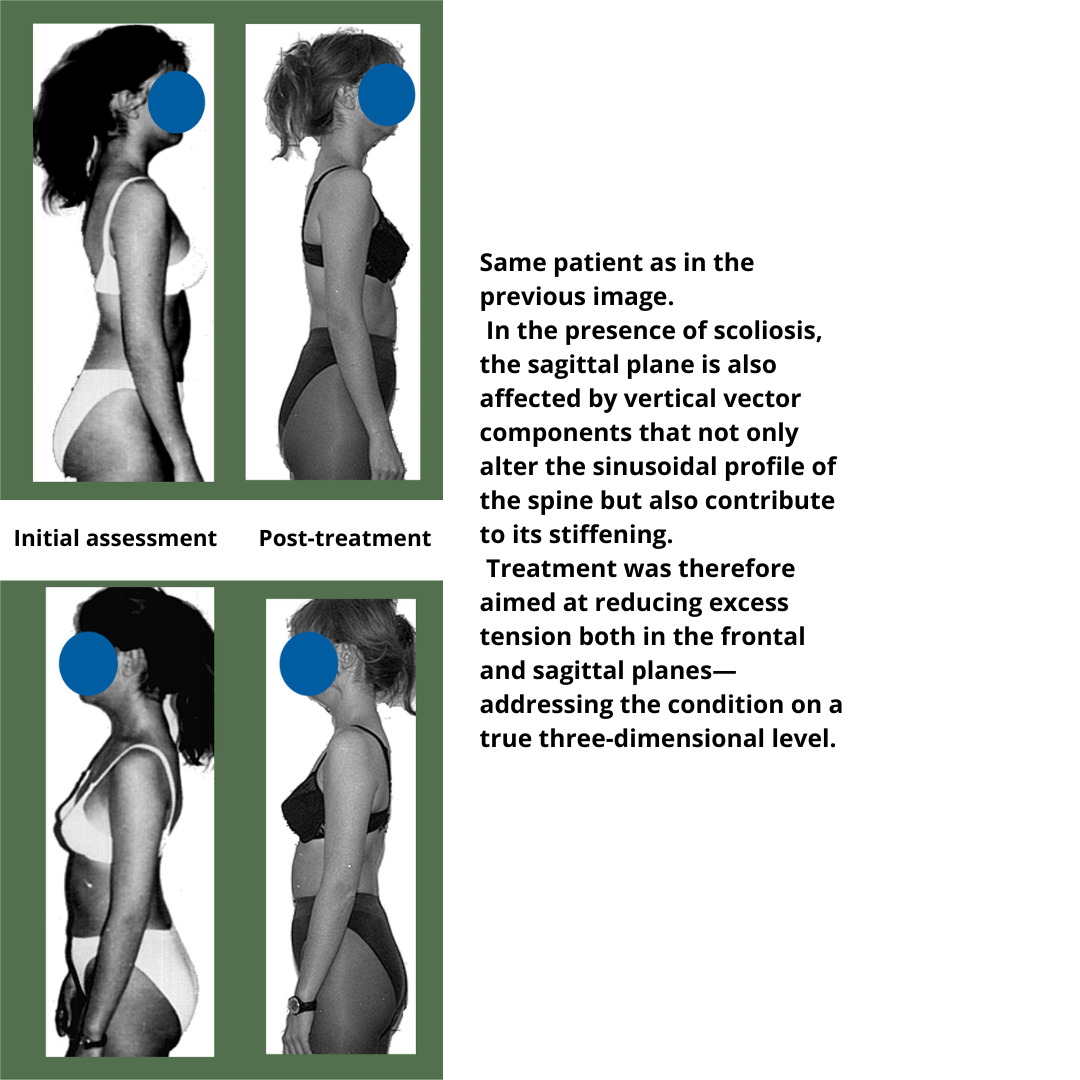
From a muscular point of view, in the sagittal plane, the balance of forces is vectorially asymmetric, leading to dominances that manifest as alterations in the skeletal trajectory of the vertebral sinusoid.
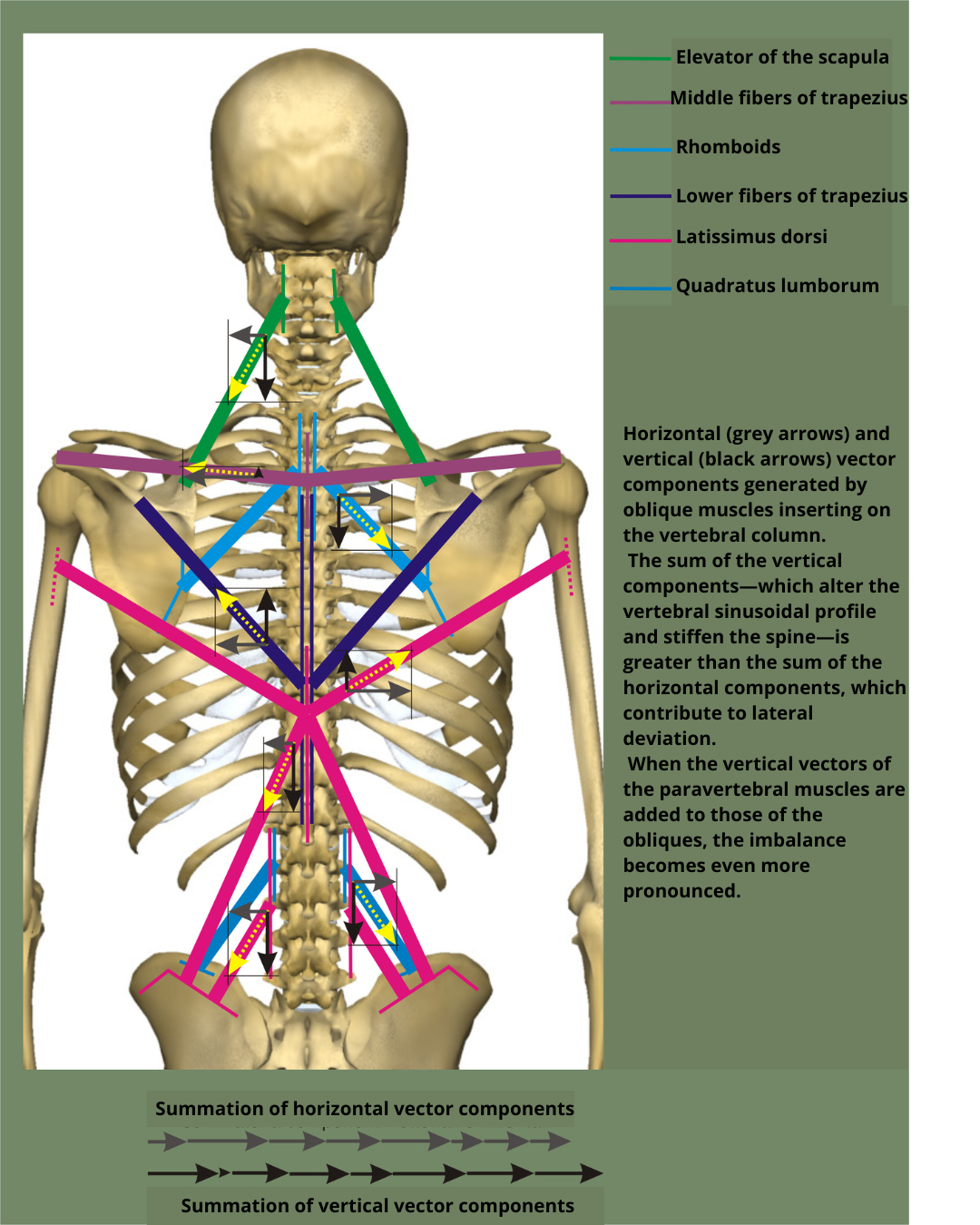
In the frontal plane, however, the horizontal components of the muscles inserting directly into the spine can be balanced by contralateral muscles with equal intensity but opposite direction. For example, the traction exerted on the thoracic vertebrae by the rhomboids can be balanced by the rhomboids of the contralateral side, potentially expressing an equal and opposite force.
In contrast to the lateral deviation of the spine, the paravertebrals, through their longitudinal vectors, stiffen the spine.
Moreover, all the oblique muscles, in addition to their horizontal components, have vertical components that, when combined with those of the paravertebrals, can modify the sagittal alignment and stiffen the spine.
In this context, the balance between the muscular forces acting upon the spine is vital for maintaining postural integrity and proper curvature across planes.
In the chapter on the neurophysiological model, it was explained how the "system" distributes muscular shortenings in a way that delays, for as long as possible, the onset of mechanical conflict within intra-articular structures—conflicts that would otherwise generate symptoms and disabling motor impairments.
From this perspective, the appearance of lateral spinal deviations can be “interpreted” as the system’s last resort, once the capacity to alter the sinusoidal sagittal profile has been saturated without triggering mechanical conflict.
In most cases, in fact, scoliosis is associated with a rigid spine and significant alterations of the sagittal alignment.
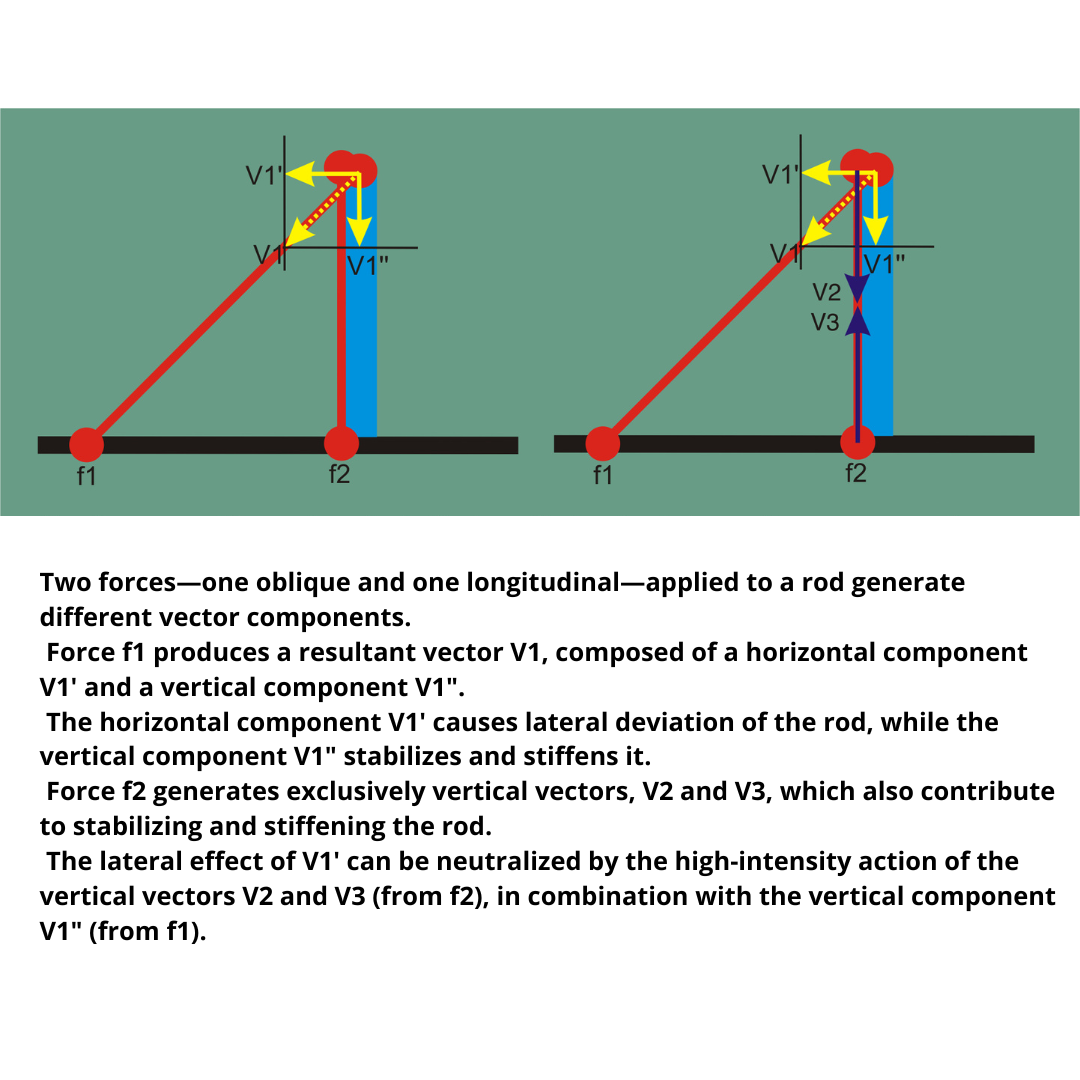
Once an oblique muscle prevails over its contralateral counterpart and causes lateral deviation of the spine, the directions of the vector components change.
If the longitudinal vector components of the muscle opposing the scoliotic deviation project beyond the midline, they combine with the horizontal and vertical components of the agonist muscle, contributing to both the stabilization and progression of the scoliotic curve.
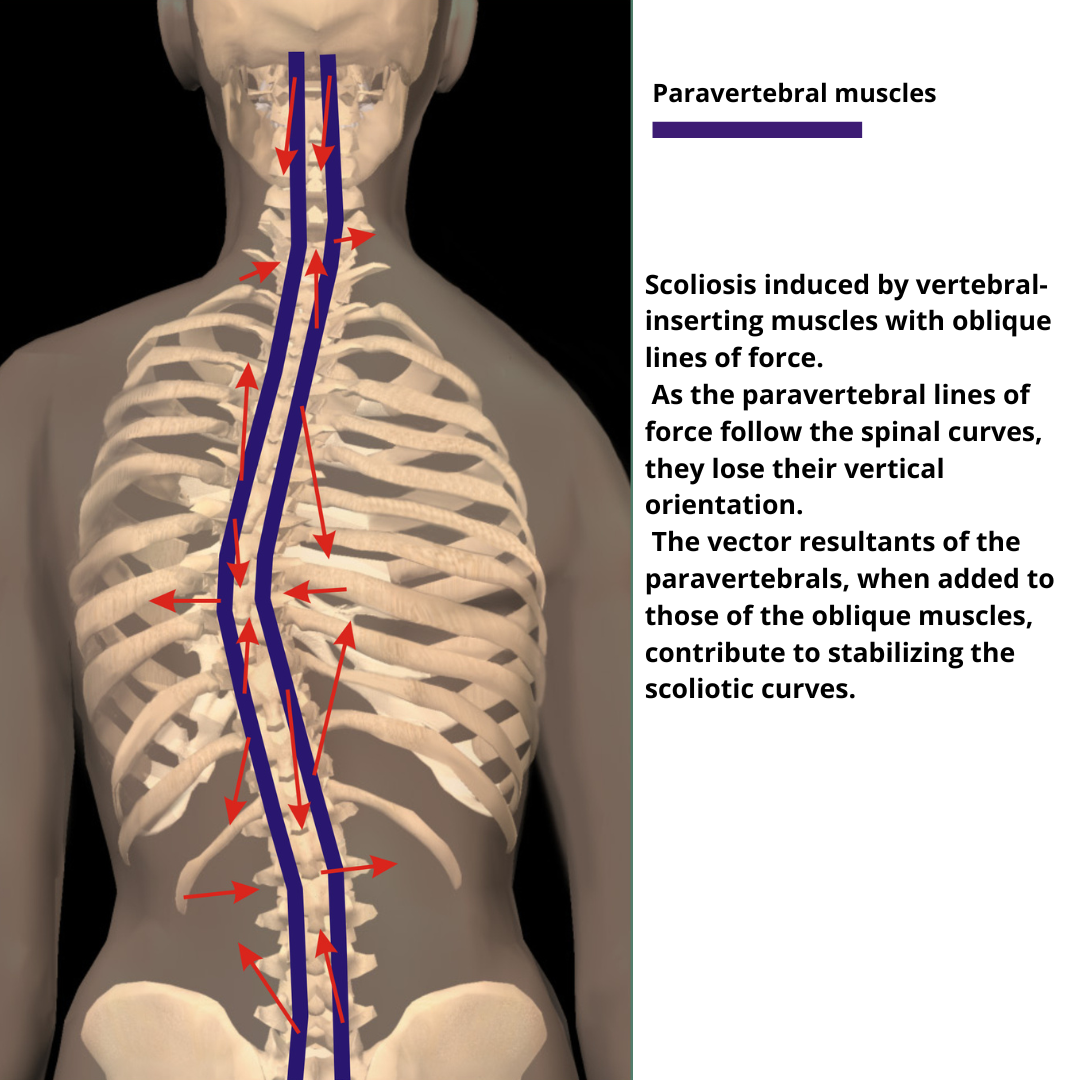
Once scoliosis has developed, the lines of force of the paravertebral muscles also change direction.
By combining with the dominant oblique forces that initiated the scoliotic pattern, they contribute to the fixation of the vertebral deviation.
The muscles on the concave side are elongated relative to their initial position, although this elongation does not exceed their maximum potential length.
These muscles develop excess tension as they attempt to counteract the lateral shift of the vertebrae. Over time, this leads to shortening of the connective portion of the muscle fibers.
Thus, although relatively elongated compared to their starting position, the concave-side muscles are, in absolute terms, undergoing a process of shortening.
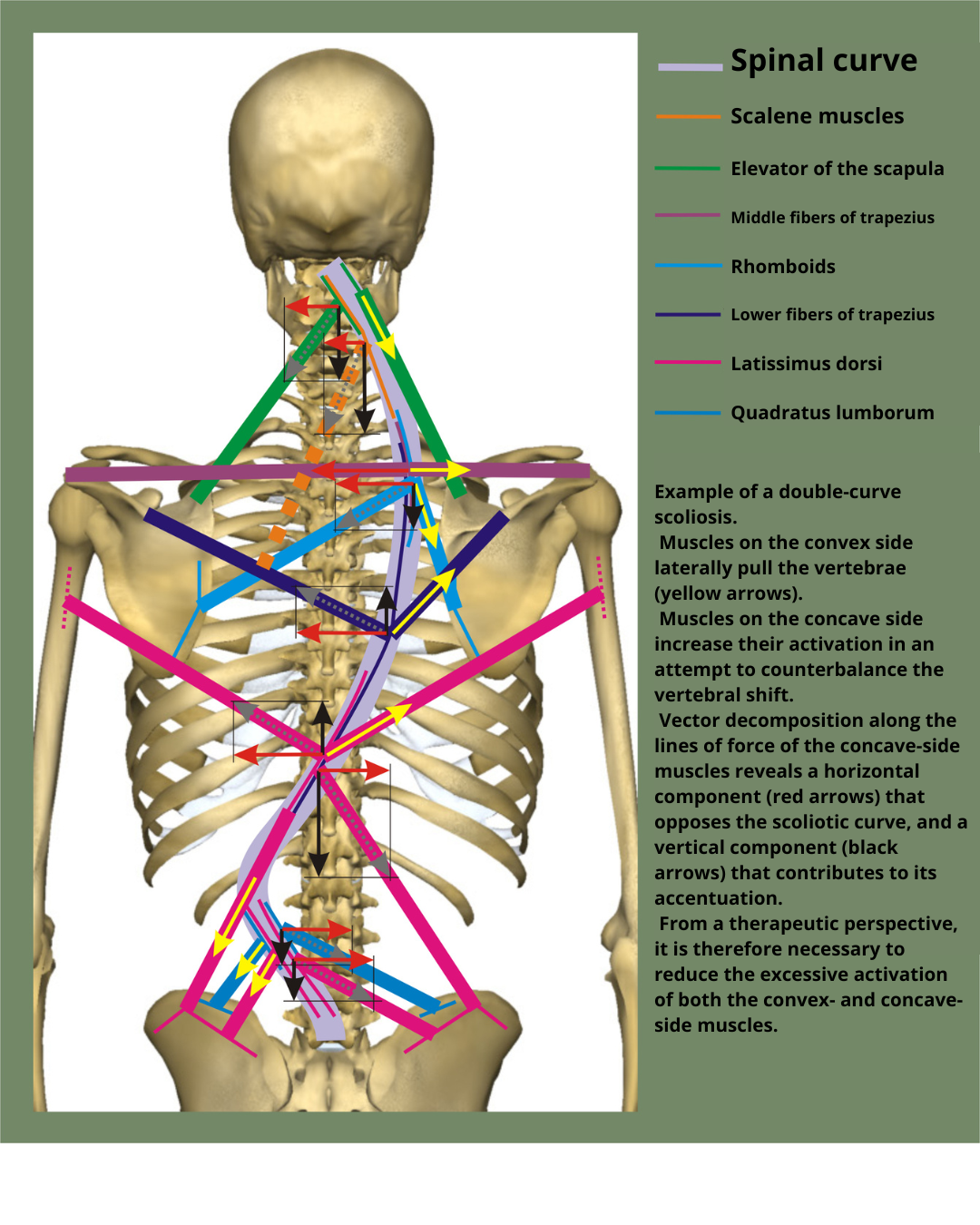
It is therefore necessary to identify which oblique vectors are dominant in generating the observed pattern.
However, treatment cannot focus solely on these, as excess tension will also involve the contralateral muscles and the paravertebral muscles.
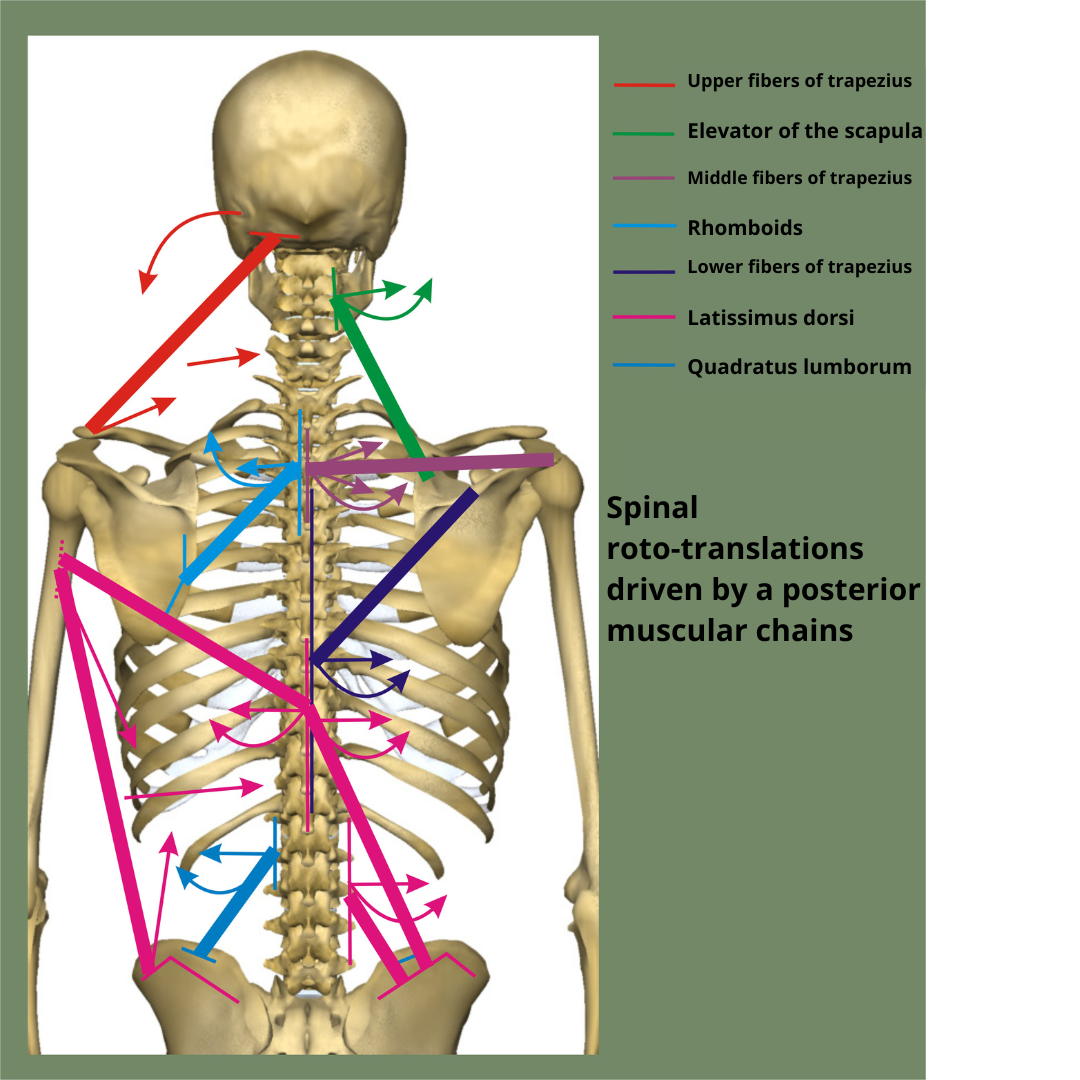
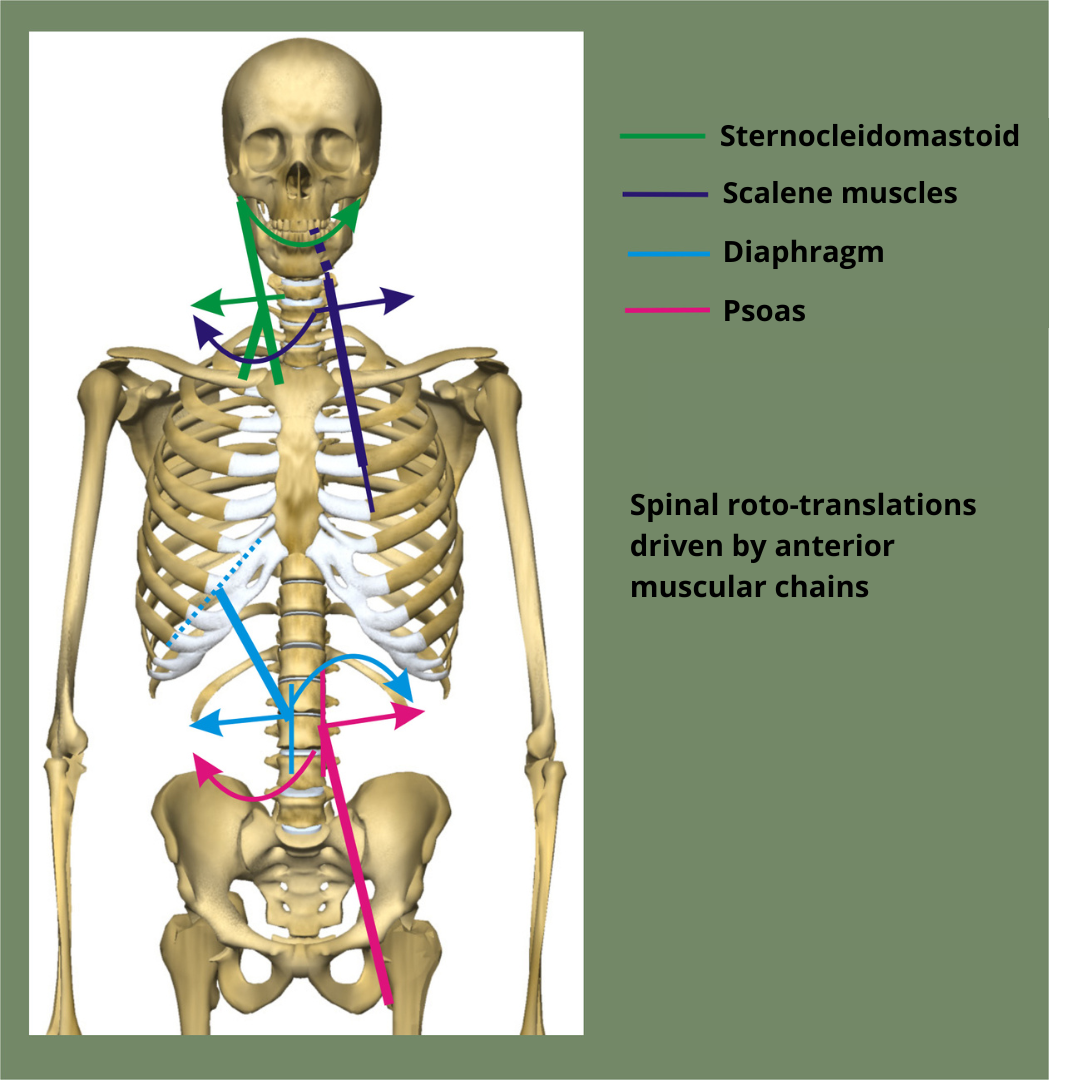
When considering individually dominant muscles from a vectorial standpoint, they may act directly on the spine—through rotation and translation (more precisely, roto-translation)—via their vertebral insertions.
Alternatively, they may induce lateral vertebral deviation as a mechanical resultant of their action on the girdles and/or the skull:
| Muscle | Direct Action | Indirect Action |
|---|---|---|
| Upper trapezius fibers | Ipsilateral head tilt and shoulder elevation | Contralateral cervico-thoracic vertebral convexity |
| Sternocleidomastoid | Ipsilateral shoulder and clavicle elevation, contralateral head rotation | Contralateral rotation of cervical vertebral bodies |
| Scalenes | Contralateral rotation of C1–C7 vertebral bodies and ipsilateral convexity | — |
| Levator scapulae | Ipsilateral convexity of C1–C4 vertebrae | — |
| Rhomboids | Ipsilateral convexity of C6–T4 vertebrae and contralateral vertebral body rotation | — |
| Middle trapezius fibers | Ipsilateral convexity of C7–T3 vertebrae and contralateral vertebral body rotation | — |
| Lower trapezius fibers | Ipsilateral convexity of T2–T12 vertebrae and contralateral vertebral body rotation | — |
| Latissimus dorsi (T7–T12 portion) | Ipsilateral convexity of T7–T12 vertebrae and contralateral vertebral body rotation | — |
| Latissimus dorsi (humerus–iliac crest portion) | Ipsilateral hemipelvis elevation and shoulder depression | Ipsilateral concavity of thoraco-lumbar vertebrae |
| Latissimus dorsi (L1–L5 portion) | Ipsilateral convexity of L1–L5 vertebrae and contralateral vertebral body rotation | — |
| Quadratus lumborum | Ipsilateral convexity of L1–L4 vertebrae and contralateral vertebral body rotation | — |
| Diaphragm | Contralateral rotation and ipsilateral convexity of L1–L4 vertebrae | — |
| Psoas | Contralateral rotation and ipsilateral convexity of T12–L5 vertebrae | — |
In the presence of scoliosis, the active muscles may be responsible for generating either the concavity, the convexity, or both, considering that the muscles on both sides are always co-contracting and act in a summative manner.
When defining the therapeutic pathway, it is therefore essential to identify the primary (first-level) vector dominances and target them initially.
As these first-level dominances diminish, secondary (second-level) dominances will become more relevant, and so on—until a satisfactory vectorial muscular rebalancing is achieved, allowing the spine to recover an optimal position in both the sagittal and lateral planes, that is, in three-dimensional space.
Core principle
The Systemic Biomechanics aims to reduce the system’s Resistant Force—which contributes to muscular rigidity and joint compression—in favor of Work Force, meaning the muscle's ability to function dynamically through elongation and coordination.
This strategy seeks to rebalance the forces acting on the spine and joints not in a flat, two-dimensional way, but through a three-dimensional perspective.
In contrast, many conventional physiotherapy approaches tend to increase the Resistant Force, which may stabilize the spine but also intensifies compressive pressure on intervertebral discs and joints.
Work Force vs. Resistant Force: an inverse relationship
These two forces behave inversely:
-
When Resistant Force increases, dynamic capacity decreases and compression rises.
-
When Work Force increases, stiffness is reduced and joint decompression improves.
Two clinical scenarios
1. Scoliosis in the developmental age
In juvenile scoliosis (adolescent or progressive idiopathic), the therapeutic dilemma revolves around strategic prioritization:
-
🟩 Increasing Work Force
-
✅ Benefit: reduces compressive loads
-
⚠️ Risk: may unmask the underlying forces driving spinal curvature
-
-
🟦 Increasing Resistant Force
-
✅ Benefit: helps stabilize the curve
-
⚠️ Risk: increases stiffness and disc pressure
-
🔎 Important note: the decision must always be made by a specialist physician, who can assess the most appropriate strategy for each case.
2. Scoliosis after skeletal maturity
In adults, the unknown causes that triggered scoliosis are no longer active. What we see are the residual structural effects of the condition.
In this case, a physiotherapy program that focuses on enhancing Work Force may:
-
improve spinal curvature
-
reduce stiffness and compression
-
enhance movement quality
Once again, the intervention should be supervised by a medical specialist to ensure clinical safety and appropriateness.
When physiotherapy can impact the curve
An often-overlooked biomechanical parameter is the relationship between lateral deviation and vertebral rotation:
-
🔁 Rotation opposite to the lateral deviation
→ Yes, muscular treatment may positively influence the curve -
➿ Rotation in the same direction as the deviation
→ No, muscular treatment is not effective in modifying the curve—scoliosis is structurally fixed
Conclusion
The Systemic Biomechanics offers a muscle-based, three-dimensional approach to scoliosis. It is particularly useful in adults and, with caution, may be considered in younger individuals. However, medical evaluation remains essential to guide physiotherapy in a safe and effective way.
Copyright © 2025 AIFiMM Formazione Mézières Provider E.C.M. n. 1701. All rights reserved.